
Submitted by Dr. Arjun J V, Written by Pendell Meyers
A man in his 50s with history of diabetes presented with acute onset abdominal pain and nausea.
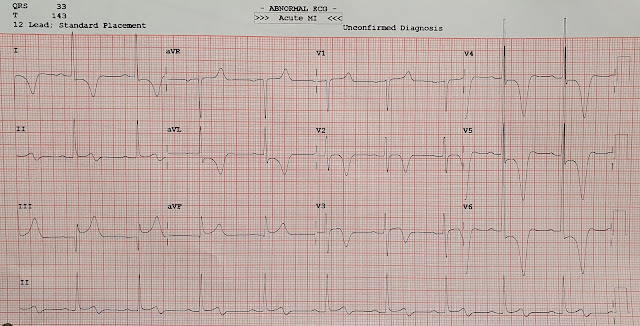
Here is his ECG at triage:
 |
| What do you think? |
Sinus bradycardia. The QRS is narrow but very abnormal with significant LVH. There are widespread, dramatic, and discordant ST and T wave deviations which are due to the LVH.
Look at leads III and aVF here for a particularly important lesson for your eyes. In these leads, the QRS does not actually have radically large QRS voltage, but yet there is substantial (easily meeting STEMI criteria) ST elevation which is due to LVH strain pattern and somewhat reciprocal to the large STD in the high lateral leads which has the perfect morphology for LVH strain pattern in I and aVL. This is an example of how sometimes a widespread repolarization abnormality may seem relatively more disproportionate in a few leads when the QRS is slightly smaller for whatever reason. I find that this is usually very important for precordial transition lead, in which the QRS may be "pulled" in both directions, sometimes making the ST segment and T wave seem concerning for that lead.
One clue to recognizing that such STE that is out of proportion to the QRS is the presence of a "saddleback". See in lead III how the R-wave and T-wave form a saddle. This is especially true when you have a saddleback in lead V2; ST Elevation with saddleback in V2 is very rarely due to OMI.
In the context of the whole ECG, with such dramatic LVH, my opinion is that all these abnormalities are attributable to the LVH, and there is no clear evidence of OMI. Likewise, the T wave inversions are not indicative of reperfusion. LVH and its associated repol abnormalities are one of the more frequent mimickers of Wellens (anterior reperfusion).
When Arjun sent this to me with minimal clinical information, I said: "No signs of OMI or reperfusion. I believe it is all due to the dramatic LVH / possibly HCM."
I showed the ECG to Dr. Smith, who immediately replied, simply: "Hypertrophic cardiomyopathy. Apical variant."
Other clues that this is not OMI are clinical: 1) the discomfort is NOT chest discomfort and thus the pretest probability of ACS is much lower and 2) the discomfort is active; Wellens waves occur AFTER the symptoms have resolved (because they are a sign of reperfusion).
Case continued:
The patient's thorough history and exam was more indicative of ureteral colic. The pain was actually in the right lower quadrant / flank and radiating to the right iliac fossa. CT confirmed a 1 cm calculus in the right ureter.
Due to the ECG findings, a formal echo was ordered which showed apical hypertrophic cardiomyopathy.
The patient was treated for the kidney stone and referred to cardiology for the incidental diagnosis of HCM.
===================================
Brief Comment by KEN GRAUER, MD (1/8/2022):
===================================
Today’s ECG shows Giant T Waves. When this is seen — Think of the differential diagnosis in Figure-1. That said — QRS amplitudes in today’s case are truly tremendous AND the patient has neither chest pain nor sign of a pulmonary embolus, recent persistent arrhythmia or neurologic disorder. Therefore, think Apical Cardiomypathy until proven otherwise. Echo will be revealing.
 |
| Figure-1: Common Causes of Giant T Waves. |
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.