This 53 yo male with no cardiac history developed chest pain 12 hours prior to admission. It was coming and going, waxing and waning, all night. At 8 AM, it increased to 9/10 and he called 911 and had this prehospital ECG recorded at 0858:
The equation value was about 30, which clearly reflects LAD STEMI. In fact, this one is so obvious (due to the ST depression) that I would not have included it in my study comparing LAD occlusion to early repolarization. The computer (which often misses MI) read it as Acute MI. The cath lab was activated prehospital.
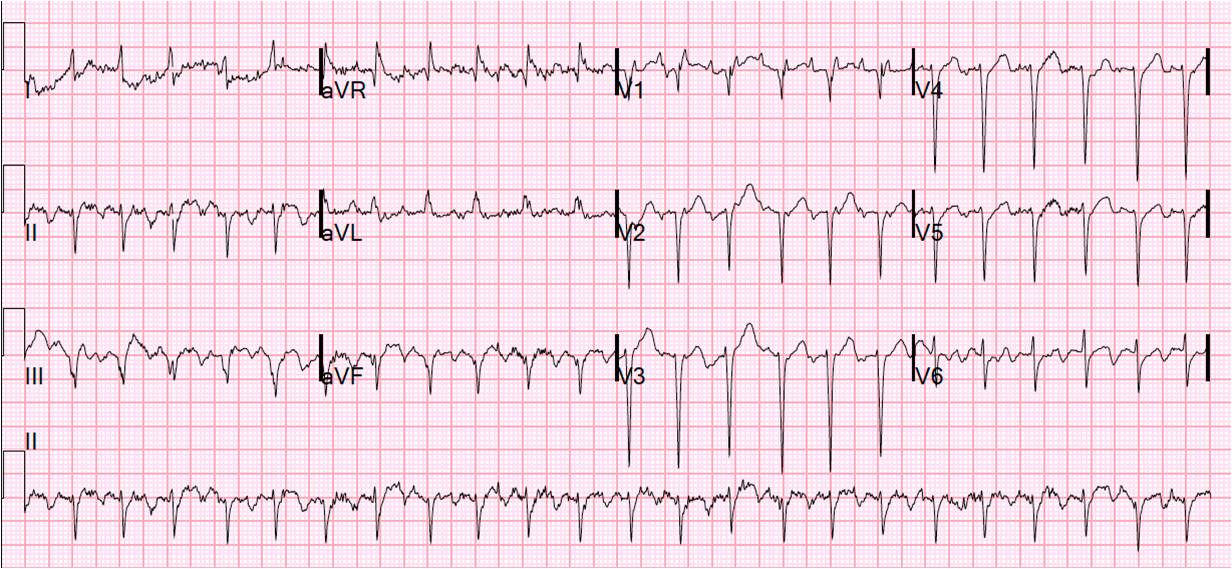
The patient received nitroglycerin and his pain greatly diminished (possibly even resolved). He arrived in the ED and had this ECG at 0947:
The initial troponin was 2.4 ng/ml. The patient went to the cath lab with a door to balloon time of 50 minutes, where he had a 4 cm long 95% narrowing of the LAD that was nitroglycerin responsive, and thought to be spasm. It was a type III (wraparound) LAD to the inferior wall, explaining the inferior ST elevation. There is no mention of thrombus. It was stented. There was also a chronically occluded circumflex and RCA which both filled via collaterals from the LAD (he was hanging on by the 5% of the LAD that was open).
Of course the ECG cannot tell you the cause of the ischemia (thrombus, spasm, or even demand ischemia), so the fact that this was spasm does not affect the ECG diagnosis, and there would be no way to know this without doing the cath.
Troponin I peaked at 82 ng/ml. Echo showed anterior and apical, and inferior, WMA and EF of 35%.
The ECG the after PCI had the same appearance, and the next day there was slightly less STE and evolving T-wave inversions, seen here:
A cardiologists called this a NonSTEMI because he saw the ST elevation as normal. Normal ST elevation, as I have shown in my study yet to be published, has an equation value that is less than 23.4 in almost all cases. But not all. Could this have been a false positive?
No. See below.
However, the troponin peaked at 82 (large MI consistent with STEMI), the convalescent echo showed a persistent anterior wall motion abnomality and a persistently poor EF of 44%.
So there was significant Myocardial wall loss, consistent with STEMI.
Finally, here is his ECG months later:
I think this pretty clearly shows that the ST elevation was not baseline ST elevation, but rather a result of the acute coronary syndrome and therefore it was indeed a STEMI.
On review, the cardiologist sees that this is a STEMI. Partly by just looking again and also because he had not seen the prehospital ECG.
Learning points:
1. ACS should be called STEMI if there is ST elevation that is a result of the ACS.
2. When there is ST elevation that is the result of ACS, there is occlusion or near occlusion of the artery.
3. The diagnosis of STEMI vs. NonSTEMI should not be based on the degree of ST elevation; rather, it should be based on whether there is ST elevation due to occlusion or near occlusion. 1 mm, or 2 mm, are arbitrary measurements that do not have a physiologic basis.
4. Many STEMIs are erroneously called NonSTEMIs.
5. If you call it a NonSTEMI, you may delay cath lab activation that should be immediate.
6. Had this patient not gone immediately to the cath lab, he would not have shown up in missed STEMI statistics. This is one reason why, in the literature, STEMI has such a low miss rate. If true STEMIs are called NonSTEMIs, then of course the STEMIs are not missed so often.
7. If the door to balloon time had been 300 minutes, this would not have been reflected in the hospital statistics. How many hospitals are accurately classifying their MI cases as STEMI? When the door to balloon time is being tabulated, how often are cases like this called NonSTEMI just to buff the statistics?
 |
| There is sinus rhythm with ST elevation in V1-V3, Q-waves in III and aVF, and ST depression in I, aVL, V5 and V6. It is obviously ACS, and, to me, clearly a STEMI. The computerized QTc is 429 and another ECG recorded shortly thereafter looked similar, with a QTc of 450. |
The patient received nitroglycerin and his pain greatly diminished (possibly even resolved). He arrived in the ED and had this ECG at 0947:
 |
| The ST elevation is somewhat less. There is now ST elevation in lead III, with reciprocal ST depression in aVL (which was also present on the prehospital, showing how aVL is more sensitive for inferior STEMI than are inferior leads). The QTc is now only 388 ms, and the equation value has dropped to 25.4 (STEMI less obvious, but still above 23.4). |
Of course the ECG cannot tell you the cause of the ischemia (thrombus, spasm, or even demand ischemia), so the fact that this was spasm does not affect the ECG diagnosis, and there would be no way to know this without doing the cath.
Troponin I peaked at 82 ng/ml. Echo showed anterior and apical, and inferior, WMA and EF of 35%.
The ECG the after PCI had the same appearance, and the next day there was slightly less STE and evolving T-wave inversions, seen here:
 |
| Persistent ST elevation in V1 and V2, with T-wave inversion in V3 - V6. |
A cardiologists called this a NonSTEMI because he saw the ST elevation as normal. Normal ST elevation, as I have shown in my study yet to be published, has an equation value that is less than 23.4 in almost all cases. But not all. Could this have been a false positive?
No. See below.
However, the troponin peaked at 82 (large MI consistent with STEMI), the convalescent echo showed a persistent anterior wall motion abnomality and a persistently poor EF of 44%.
So there was significant Myocardial wall loss, consistent with STEMI.
Finally, here is his ECG months later:
 |
| Most ST elevation is gone, equation value is now 22.1 (less than 23.4), and the R-wave in V4 has recovered some. |
On review, the cardiologist sees that this is a STEMI. Partly by just looking again and also because he had not seen the prehospital ECG.
Learning points:
1. ACS should be called STEMI if there is ST elevation that is a result of the ACS.
2. When there is ST elevation that is the result of ACS, there is occlusion or near occlusion of the artery.
3. The diagnosis of STEMI vs. NonSTEMI should not be based on the degree of ST elevation; rather, it should be based on whether there is ST elevation due to occlusion or near occlusion. 1 mm, or 2 mm, are arbitrary measurements that do not have a physiologic basis.
4. Many STEMIs are erroneously called NonSTEMIs.
5. If you call it a NonSTEMI, you may delay cath lab activation that should be immediate.
6. Had this patient not gone immediately to the cath lab, he would not have shown up in missed STEMI statistics. This is one reason why, in the literature, STEMI has such a low miss rate. If true STEMIs are called NonSTEMIs, then of course the STEMIs are not missed so often.
7. If the door to balloon time had been 300 minutes, this would not have been reflected in the hospital statistics. How many hospitals are accurately classifying their MI cases as STEMI? When the door to balloon time is being tabulated, how often are cases like this called NonSTEMI just to buff the statistics?