
Written by Willy Frick
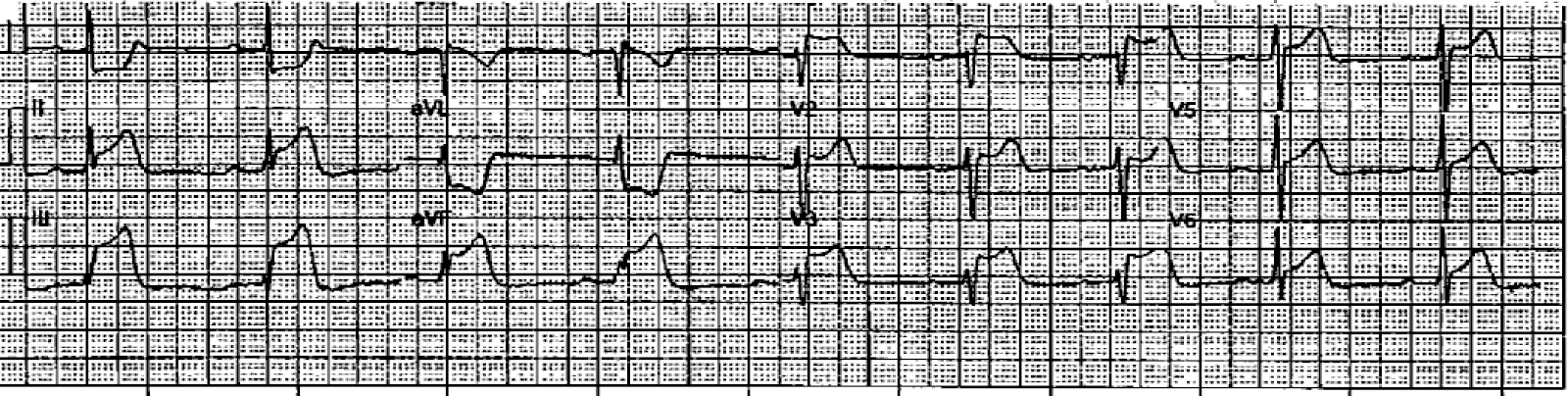
A man in his early 40s with prior anterior OMI s/p bare metal stent to LAD in 2014 presented with acute chest pain, nausea, dyspnea, and diaphoresis. He was brought in by EMS. His first ECG is shown:
ECG 1
 Obvious STEMI (+) OMI. What would you guess is the culprit?
Obvious STEMI (+) OMI. What would you guess is the culprit? There is STE in V1 and V2 with lateral STD, a pattern known as precordial swirl, so...it should be LAD, right? Sure, there's evidence of ischemia in lead III (and aVF to a lesser degree), but many patients have a long "wraparound" LAD that supplies the distal inferior wall producing inferior STE when occluded.
I sent this ECG to several different friends separately, and everyone said it was suspicious for proximal RCA occlusion with right ventricular infarction. This may be a surprise to many, who are used to thinking of V1-V6 as the anterolateral leads. And used to thinking of RCA as supplying the inferolateral wall.
But remember that V1-2 especially are rightward looking leads. Think of this image:
Figure 1: Schematic representation of V1 and V2 electrodes

This is a transverse CT. The four cardiac chambers are labeled (LA, RA, LV, RV). The right ventricle is the most anterior chamber, and V1 and V2 electrodes are overlying. This is why we see:
- T wave inversion in the right precordial leads from acute PE
- Epsilon waves in V1 and V2 due to right ventricular pathology in ARVC
- Large R waves in V1 from right ventricular hypertrophy
Nanashī educated me about the term "pseudoanteroseptal" injury pattern of proximal RCA occlusion (since embarrassingly, I had not read this post). For me, the key to this ECG is the STE maximal in V1 indicating a very rightward vector of injury. This is corroborated by STE in III, whereas there is STD in II.
Because of the obvious presentation and STEMI (+) ECG, the patient was immediately taken to cath lab. In fact, everything was highly efficient, and exactly 20 minutes after he arrived in the hospital, he had his first angiogram!

Figure 2: LAO cranial angiogram, annotated on the left, unedited on the right

But, does diagonal culprit fit with the ECG?
Answer: No.
Our differential was most likely proximal RCA versus possible LAD due to the finding of precordial swirl with massive STE in V1. If LAD produces a swirl pattern, it should be due to involvement of the septal perforators. The diagonal vessel does not give septal perforators, so it should not cause swirl. Diagonal culprits classically cause South African Flag pattern with STE in I, aVL, and V2 with reciprocal STD in III.
The cardiologist then worked meticulously on the diagonal, which was a difficult intervention. The vessel was difficult to wire and required multiple attempts. There were also several other technical challenges including difficulty passing the intravascular ultrasound probe. Additionally, the ostial location of the lesion adjacent to a pre-existing LAD stent (not well seen in the angiogram) added complexity. Although the initial ballooning was quite rapid and well within the 90 minute target, the final post-intervention angiogram of the diagonal vessel was about two and a half hours after the patient arrived.
At that point, the first injection of the RCA was performed.
Figure 3: TIMI 0 proximal RCA

Unfortunately, this image of the culprit was taken 152 minutes after arrival. I made a video explaining the post intervention angiogram for those who are interested.
So although the recorded "door to balloon time" is 43 minutes, this number describes an irrelevant consideration -- time to revascularize a non-culprit lesion. Considering the RCA as the culprit, the door to balloon time was instead 157 minutes.
Echocardiogram showed mild inferior hypokinesis with overall preserved LVEF, 60%. There was evidence of RV dysfunction. (For the echocardiographically inclined, TAPSE was 1.4 cm.) Troponin prior to the cath was within the reference range, and there was no repeat measurement. Fortunately, the patient did well clinically in spite of the delay.
Learning points:
- For OMI with STE maximal in V1, RV infarct is likely
- Wrong vessel intervention is VERY common, perhaps more frequent than 1 out of 4
- STEMI metrics frequently conceal missed opportunities for process improvement
Here is a related Case, explained by video:
Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion
This is a video I made a while back. I thought it was worth a re-post. For those who don't have time to watch a video, you'll have to read the ECG as shown on this still frame because I lost it and cannot post it.
See down below for explanation if you don't want to watch the video.
See down below for explanation if you don't want to watch the video.
There is inferior STEMI. But there is also ST elevation in leads V1 and V2. When you see this, think right ventricular (RV) MI. The hypotension is further evidence for RV MI. There was no right sided ECG.
I heard about the case, and saw the ECG, shortly after the patient left for the cath lab. I called the interventionalist while the patient was on the table and he told me that the occlusion was not in the proximal RCA, but further down. I asked if he was sure about this, because the ECG would indicate a proximal RCA occlusion with RV MI. He took another look and realized that the culprit was indeed in the proximal RCA and that the thrombus had embolized distally. And so he put the stent in the proximal RCA.
Learning point: Even when you have an angiogram, the ECG findings make a difference.
I heard about the case, and saw the ECG, shortly after the patient left for the cath lab. I called the interventionalist while the patient was on the table and he told me that the occlusion was not in the proximal RCA, but further down. I asked if he was sure about this, because the ECG would indicate a proximal RCA occlusion with RV MI. He took another look and realized that the culprit was indeed in the proximal RCA and that the thrombus had embolized distally. And so he put the stent in the proximal RCA.
Learning point: Even when you have an angiogram, the ECG findings make a difference.
More Cases of Pseudoanteroseptal MI:


A 40-Something male with a "Seizure," Hypotension, and Bradycardia

Pseudoanteroseptal STEMI in the Setting of Paced Rhythm (published by me in JAMA Internal Med)

===================================
MY Comment, by KEN GRAUER, MD (6/17/2025):
===================================
- In a patient with new symptoms — ST elevation in lead V1 merits inclusion of acute RV MI in the differential diagnosis. As per Dr. Frick — the principal differential diagnosis of today's initial ECG (that I've reproduced in Figure-1) is: i) Acute proximal RCA occlusion with RV MI; — vs — ii) Acute proximal LAD occlusion ("Swirl" pattern).
- "A picture is worth 1,000 words". Acute RV MI becomes especially likely when the ECG looks like the tracing shown in Figure-1 because: i) Chest lead ST elevation is limited to leads V1 and V2, in which the amount of ST elevation is marked in lead V1 (more than 6 mm!) — greater in lead V1 than in V2 — and not seen beyond lead V2 (whereas LAD OMI usually has ST elevation in additional anterior leads); — and, ii) The ST elevation with Q wave and terminal T wave inversion in lead III (but not in the other inferior leads) indicates associated inferior OMI — and — a rightward ST elevation vector consistent with RV MI.
- The combination of acute inferior OMI and RV MI implicate the proximal RCA (Right Coronary Artery) as the "culprit" artery.
- When the possibility of acute RV MI is raised — Get right-sided leads! This apparently was not done in today's case.
- Awareness of the likelihood of acute RV MI based on the ECG in Figure-1 (and therefore of the proximal RCA as the likely "culprit" artery site) — provides an excellent example of how superior ECG interpretation can aid the angiographer in knowing where to look for the site of acute occlusion. Had the significance of the above-described ECG findings been recognized — myocardial-preserving PCI could have been accomplished 2 hours sooner than it was.
- Elsewhere on ECG #1 — diffuse ST depression + ST elevation in lead aVR (albeit to a lesser degree than that seen in leads V1,V2) — is consistent with DSI (Diffuse Subendocardial Ischemia) and this patient's history of underlying coronary disease (ie, his prior LAD stent in 2014).
- Finally — the failure to recognize the probable "culprit" artery from the ECG in Figure-1 led to initial wrong-vessel intervention in today's case — which as per Dr. Frick, led to misclassification of "door-to-balloon" time as "appropriate" in chart records (whereas "door-to-balloon time" of the correct culprit artery was significantly delayed).
-USE.png) |
| Figure-1: The initial ECG in today's case. |
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.