
4916132
A 50-something male smoker with h/o Diabetes, but with no cardiac history presented by ambulance with acute chest pain. It was described as severe, pleuritic, with radiation to bilateral shoulder blades, and associated with shortness of breath. Constant. He had never had this before.
His chest wall was exquisitely tender and palpation exactly reproduced his pain.
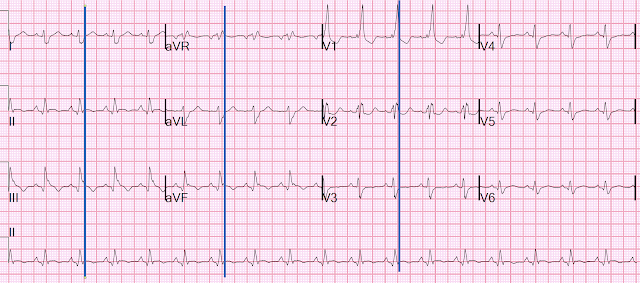
He had this prehospital ECG.

There is a right bundle branch block, and also right axis deviation due to left posterior fascicular block. An old ECG was available that did not have BBB of any kind, but a more recent ECG description from an outside hospital stated "RBBB and LPFB".
There are inferior Q-waves, and also coved (convex) minimal STE in lead II, with downsloping minimal STE in III and aVF, with inverted T-waves, with only a trace amount of reciprocal STD in aVL, which I could not see well at the time but I can see when I magnify it:

So this was very suspicious for acute OMI.
But I was suspicious that it might be an unusual OMI mimic because of:
1) the downsloping ST segments and the inverted T-wave, in the context of RBBB + LPFB, and also
2) that chest wall palpation exactly reproduced the pain.
So we immediately recorded an ED 12-lead (higher quality tracing):

Due to the artifact on the above tracing, this tracing was printed out 7 seconds later:

We activated the cath lab.
Bedside POCUS showed overall poor function and multiple wall motion abnormalities.
First hs Troponin I returned much later at 12,186 ng/L. This very high initial troponin indicates that the infarct was not acute, even if the symptoms were.
Angiographic findings:
1. Left main: small caliber with mild distal tapering (30%).
2. LAD: severe 90% mid stenosis at the bifurcation of a diagonal branch.
3. LCX: non-dominant, small caliber. It supplies a bifurcating OM. The OM has diffuse disease with stenosis up to 60%. The caliber is relatively small.
4. RCA: This is thrombotically occluded in the mid segment (TIMI 0 flow). It supplies an RPDA (right posterior descending artery) and large RPLA (right posterolateral artery) that have luminal irregularities. This was opened and stented.
There is a second LPLA (Posterolateral) that is chronically occluded.
(Other lesions were stented 2 dyas later.)
Note: although many object to the use of "posterior" for infarcts, since Bayes de Luna showed by MRI that "posterior" infarcts are in the lateral myocardial wall, I continue to use "posterior" because it faces the posterior wall of the chest and only manifests as anterior ST depression, NOT as lateral ST elevation. Here you can see that interventionists use the term "Posterior" for branches of the coronaries. The term "posterior" is appropriate!!
Next morning:

Let's put in lines that show the end of the wide QRS, so we know where the ST segment begins.
Formal Echo:
Decreased left ventricular systolic performance; estimated left ventricular EF is 50%.
Normal left ventricular cavity size with mild concentric left ventricular hypertrophy.
Regional wall motion abnormality
- apex, distal septum, anterior, lateral and inferior segments.
- mid to basal inferior.
The patient later went
Learning Points:
1. A high percentage of MI patients have chest wall tenderness, up to 25% in some studies.
2. Downsloping ST Elevation may indeed by due to acute OMI, (or subacute in this case). This seems to be especially in the case of fascicular block (unverified anecdotal observation of mine). The majority of ECGs with acute LAD or Left Main OMI which I have seen have downsloping ST Elevation. See below.
Here are a few of the first examples which come up by clicking on the RBBB and LAFB label on my blog:
A woman in her 60s with 6 hours of chest pain, dyspnea, tachycardia, and hypoxemia

Here is another proven left main occlusion in a young woman who presented with sudden pulmonary edema, had this ECG recorded, then arrested and was resuscitated after 30 minutes of CPR:

What is the Diagnosis in this 70-something with Chest Pain?

Ventricular Fibrillation, ROSC after perfusion restored by ECMO, then ECG. Protocols can be overridden by Physician Judgment.

No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.