
An elderly woman was found to be bradycardic. She was awake with a BP of 120/70.
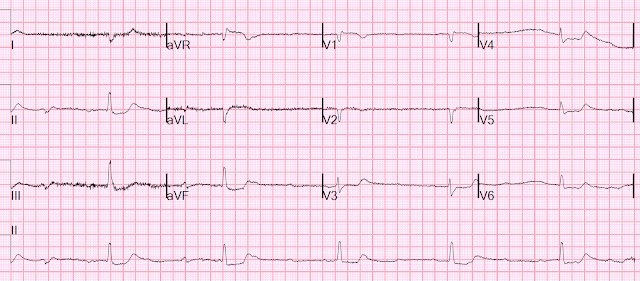
Here is her prehospital ECG:

What do you think?
I thought this was likely due to hyperkalemia. I do not see P-waves. It appears to be sinus arrest with ventricular escape. The ST deviations could be ischemia, but are very often the result of hyperkalemia.
First ED ECG:

Pretty much the same
She was given multiple doses of Calcium gluconate. 6 grams as I recall.
And another ECG was recorded 9 min later:

3rd 2.5 hours later
There are some possible P-waves here, but if they are, there is complete AV block as well, with continued ventricular escape.
We continued giving calcium. We also gave insulin, D50, IM terbutaline 0.25 mg (beta-2 agonist), 80 mg of furosemide.

Here lactate returned at 8.5, K 7.4, Cr 2.9
Later, after 21 g of calcium and more shifting, the K was down to 5.8.
This ECG was recorded:
There is now an atrial rate of about 100 with complete AV block and a probable ventricular (vs. junctional) escape that is much narrower.
So in spite of massive management of hyperK, the complete AV block persisted.
The patient was made comfort care only, and there was no further management.
Learning Points
1. Bradycardia and AV block can be caused by Hyperkalemia.
2. There can be simultaneous AV node disease and hyperkalemia.
3. If the AV block does not resolve with management of hyperkalemia, then there is underlying intrinsic AV node disease.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.