Here are some basic concepts before we get into the ECGs:
- STEMI and NonSTEMI are arbitrary terms that may confuse the clinician.
- "STEMI" should mean "coronary occlusion" (or near occlusion, without good collateral circulation -- in other words, it needs thrombolytics or emergent angiogram with PCI).
- NonSTEMI should mean "MI without occlusion."
- "STEMI-equivalent" is a good term for "coronary occlusion".
- Many STEMI-equivalents have no significant ST elevation, as you may have seen from many of my posts.
- In some STEMI-equivalents (posterior STEMI, lateral STEMI, posterolateral STEMI), ST depression is the only, or most visible, feature of the ECG.
- So how do we tell if ST depression represents a STEMI-equivalent or NonSTEMI/subendocardial ischemia?
- As I see it, there are 5 primary patterns of ST depression. I outline them below and demonstrate them to show which are STEMI equivalents and which are NonSTEMI.
- NonSTEMIs/subendocardial ischemia may need immediate angiogram and PCI (or emergent CABG) if the patient is hemodynamically unstable or if the ischemia (as measured by chest pain and ECG findings) cannot be controlled medically (aspirin, GP IIb IIIa inhibitor, antithrombotic, nitroglycerin).
- NonSTEMIs should never get thrombolytic therapy.
- Clopidogrel should probably be avoided in NonSTEMIs that have a high likelihood of needing CABG (ST elevation in aVR)
ST elevation axis (vector) is the opposite of the ST depression vector, though not necessarily the same magnitude (millivolts or millimeters). Once you understand this, it makes everything simple. It is worth a few moments to concentrate and learn it.
First, there are countless ways ischemic ST depression (STD) presents.
Check here, for instance.
But I like to classify 5 primary STD patterns in ACS in which there is
ST depression without any significant ST elevation. Some are STEMI-equivalents, and some are Non-STEMI. The diagnosis depends on the
ST axis. Which direction does ST elevation go? Sometimes it is better to ask: what is the opposite of the ST
depression vector?
If the ST depression is directly anterior (V1-V4), then the ST elevation axis is directly posterior, and there is a high likelihood of posterior STEMI.
If the ST depression vector is inferior and leftward, there is a lot of ST depression in inferior and left lateral leads, and corresponding ST elevation in aVR (superior and rightward), towards the base (top) of the heart. (There may also be ST elevation in right sided leads but NOT due to RV MI).
Unless there is a concomitant anterior STEMI (high occlusion resulting in STEMI of anterior and basal walls), STE in aVR is not a STEMI in lead aVR; rather the STE in aVR is reciprocal to a leftward and inferior ST depression axis caused by diffuse subendocardial ischemia.
- Thus, an ST elevation axis that is anterior, posterior, inferior, or left lateral is likely to be a STEMI-equivalent. Anterior-Superior axis (anterior STE + V1 and aVR) is also STEMI
- An ST axis which is rightward (ST depression V3-V6) or superior (ST elevation in aVR) is likely to be a NonSTEMI.
In all this, it is important to realize that
ST depression does not localize subendocardial ischemia. On the other hand,
reciprocal ST depression does help to localize the area with ST elevation.
For instance, if there is ST depression in V4-V6, it does not necessarily mean that the ischemia is of the lateral wall. The ischemia
might be in that location, but not necessarily.
This is a mystery I cannot explain, but has been proven by comparing ECG findings to angiography.
Examples
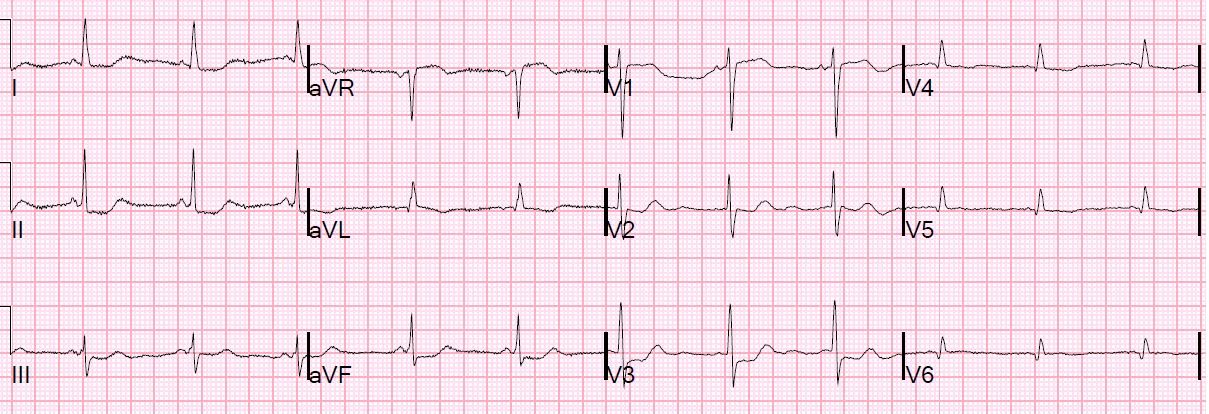
1. Severe subendocardial ischemia, nonlocalized: Diffuse ST depression, including leads I, II, aVF, III, V3-V6, with
STE in aVR. This one was
severe acute left main stenosis. One might also find this in severe 3 vessel disease with ACS.
A patient who lives through Left Main
Occlusion is not common. Acute left main ACS with critical stenosis is the much more common issue, and this causes subendocardial ischemia. So no thrombolytics. Both severe 3 vessel ACS and acute left main ACS are likely to need CABG and thus you might want to avoid clopidogrel. So the fact that 3 vessel ACS and left main cannot be differentiated on the ECG is not so important.
 |
| ST elevation is in aVR. The ST axis is towards aVR, but this does not mean there is STEMI in aVR! Instead, this elevation is reciprocal to global subendocardial ischemia with the negative ST axis inferior and lateral, towards the apex (I, II, aVF, III, V3-V6). There is no occluded artery here. There is no STEMI. The precordial ST depression is not maximal in precordial leads V1-V4, therefore there is no posterior ST axis and no posterior STEMI. |
|
2. Isolated posterior STEMI: Leads V1-V4 primarily
Standard 12-lead ECG:
 |
ST depression is limited to precordial leads and is maximal in V2-V4 precordial leads. Thus the ST axis is posterior.
|
|
Posterior ECG: Leads V4-V6 replaced by leads V7-V9:
 |
| ST elevation in V7-V9 confirms posterior STEMI. There was a circumflex occlusion. |
|
3. Posterolateral STEMI: Precordial leads V1-V3 +/-V4 with STD in II, III, aVF, but no ST depression in I and minimal STE in aVL
Example 1:
 |
| The ST axis is away from inferior and anterior leads, and so is posterior and superior. With a bit of ST elevation in aVL, it is also lateral. |
|
Example 2:
 |
There is ST Elevation here, in aVL, but it is much less obvious than the ST depression in inferior leads and in V2, V3.
|
|
4. Subendocardial ischemia, non-localized, usually not as severe as #1 above: ST Depression in V3,V4-V6. ST axis is rightward, with little posterior or inferior components.
 |
77 yo presented with pulmonary edema. Troponin I peaked at 6.7 ng/ml. There was an inferoposterior wall motion abnormality. All arteries were diseased but there was no obvious culprit. This is not a posterior STEMI. This is a NonSTEMI.
|
|
In this case, the ST axis is perpendicular to III and aVF and towards aVR, and away from I and II (leading to ST depression in I and II). So it is upward and rightward. If this were inferior STEMI, the ST axis would be towards III and aVF (which also give ST depression in I and aVL).
5. Isolated High Lateral STEMI: II, III, aVF only (ST Depression is reciprocal to minimal STE in aVL)
Example 1.
 |
Acute Circumflex occlusion (also old inferior MI with Q-waves, and early repol giving anterior STE)
|
|
Example 2.
 |
Acute First Diagonal Occlusion.
|
|
Example 3.
 |
| This patient presented with DKA and an acute STEMI with first diagonal occlusion. The peaked T-waves are due to hyperkalemia, which was immediately treated. Notice that the ST elevation in aVL is far less obvious than the reciprocal ST depression in II, III, aVF. The ST axis is towards aVL and away from inferior leads; thus there is ST depression in inferior leads. There was a 100% acute occlusion of the first diagonal, with peak troponin I of 110 ng/ml, new lateral wall motion abnormality, and ejection fraction decreased to 55%. |