
See 6 even better cases of T-wave pseudonormalization here.
Here is another case. Do not miss this one:
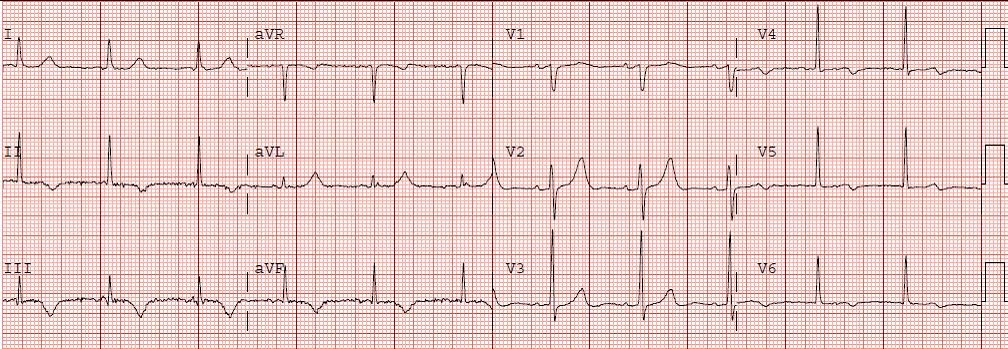
This 64 year old woman presented intoxicated with nausea and vomiting and epigastric pain, with no chest pain. She has a history of a stent, but unknown in which artery. She stopped taking clopidogrel 2 weeks ago because she ran out. Here is the initial ECG; there was no previous ECG for comparison.

Notice there is deep symmetric T inversions in inferior leads, and a large upright T wave in aVL. There is also some T inversion laterally. This is all suggestive of inferior (and lateral?) Non-STEMI, due to reperfused RCA or circ. Inverted T waves are also known as "reperfusion" T-waves. If they are in the anterior leads, they are often referred to as "Wellens' T-waves."
A troponin returned elevated, and a repeat ECG was recorded:

Now the inferior T-waves have become mostly upright, in this case biphasic. There is some ST elevation, but it is not quite 1 mm in two consecutive leads. There is new ST elevation in lead V1, which in this context is diagnostic of right ventricular STEMI.
This phenomenon is called "pseudonormalization of T-waves" because normal T-waves are upright (same axis as QRS), but become inverted in non-STEMI that is reperfused. They become deceptively upright (not normal, but "pseudo" normal) when the artery re-occludes. Thus, where reperfusion of the infarct-related artery (IRA) leads to T-wave inversion, if inverted leads become suddenly upright, this is diagnostic of re-occlusion of the IRA.
There is nothing magical about 1 mm of ST elevation. ST elevation is used as a very imperfect surrogate for coronary occlusion. Coronary occlusion that does not spontaneously reperfuse or is not compensated for by collateral circulation will quickly lead to irreversible myocardial loss. Reperfusion therapy is indicated for occlusion, even when there is not 1 mm of STE in 2 consecutive leads. However, the specificity of the ECG for occlusion becomes less as the STE is less. So expertise in interpreting the ECG is particularly important for these cases.
In this case, it was clear that there was a very unstable thrombus in the RCA or circ, and that if it was not 100% occlusive, it was very nearly so.
The cath lab was activated, a 100% proximal RCA stent thrombosis was seen and the artery was opened.
This also illustrates how chest pain or even discomfort may be completely absent in STEMI. Below is the post-cath ECG, showing T-waves are now inverted again (indicating reperfusion).

Here is another case. Do not miss this one:
A Middle-Age Male with Chest Pain that Recurs in the ED
This 64 year old woman presented intoxicated with nausea and vomiting and epigastric pain, with no chest pain. She has a history of a stent, but unknown in which artery. She stopped taking clopidogrel 2 weeks ago because she ran out. Here is the initial ECG; there was no previous ECG for comparison.
Notice there is deep symmetric T inversions in inferior leads, and a large upright T wave in aVL. There is also some T inversion laterally. This is all suggestive of inferior (and lateral?) Non-STEMI, due to reperfused RCA or circ. Inverted T waves are also known as "reperfusion" T-waves. If they are in the anterior leads, they are often referred to as "Wellens' T-waves."
A troponin returned elevated, and a repeat ECG was recorded:

Now the inferior T-waves have become mostly upright, in this case biphasic. There is some ST elevation, but it is not quite 1 mm in two consecutive leads. There is new ST elevation in lead V1, which in this context is diagnostic of right ventricular STEMI.
This phenomenon is called "pseudonormalization of T-waves" because normal T-waves are upright (same axis as QRS), but become inverted in non-STEMI that is reperfused. They become deceptively upright (not normal, but "pseudo" normal) when the artery re-occludes. Thus, where reperfusion of the infarct-related artery (IRA) leads to T-wave inversion, if inverted leads become suddenly upright, this is diagnostic of re-occlusion of the IRA.
There is nothing magical about 1 mm of ST elevation. ST elevation is used as a very imperfect surrogate for coronary occlusion. Coronary occlusion that does not spontaneously reperfuse or is not compensated for by collateral circulation will quickly lead to irreversible myocardial loss. Reperfusion therapy is indicated for occlusion, even when there is not 1 mm of STE in 2 consecutive leads. However, the specificity of the ECG for occlusion becomes less as the STE is less. So expertise in interpreting the ECG is particularly important for these cases.
In this case, it was clear that there was a very unstable thrombus in the RCA or circ, and that if it was not 100% occlusive, it was very nearly so.
The cath lab was activated, a 100% proximal RCA stent thrombosis was seen and the artery was opened.
This also illustrates how chest pain or even discomfort may be completely absent in STEMI. Below is the post-cath ECG, showing T-waves are now inverted again (indicating reperfusion).

Steve did this patient have a previous EKG with which to compare to the first EKG ?
ReplyDeleteRobert,
ReplyDeleteThere was no previous ECG available for comparison.
Steve Smith
Dr. Smith,
ReplyDeleteI am a first year cardiology fellow in Chicago and find your blog extremely useful. Of course, we read books and interpret ecgs all the time, but your cases and your insight is so much more in depth than what a book can teach you. Only years of experience and expertise can impart the type of knowledge and insight that your analysis in your blog teaches.
Thank you so much for this awesome blog and all of your expertise. Many generations of future physicians will benefit from your blog.
I appreciate the comments. Thank you!
ReplyDeleteI have a few questions:
ReplyDelete1. How do you differentiate these reperfusion inverted T waves from other causes of TW inversions (eg PE, Metabolic, Persistent/Benign juvenile TW Inversion)
2. Would you have activated the cath lab based on first ECG and dicey clinical symptoms (no chest pain) without the second ECG and the Trop?
3. Reperfusion Inverted T waves either on inferior leads or Wellens -- are they the same reperfusion "upright" T waves on posterior MI?
As usual, thanks
JD
1. Complex question, too long to answer here. Please read my chapter on this (chapter 15) in: Brady WJ and Truwitt DT, Critical Decisions in Emergency and Acute Care Electrocardiography, p. 103, or chapter 8 in my "The ECG in Acute MI: An Evidence-Based Manual of Reperfusion Therapy", or my chapter in EM Clinics of N Am 24(1):53-89 (T waves on pp. 64-69) or the next chapter in the same issue, or the Text "ECG in Emergency Medicine and Acute Care (Chan, Brady, etc), my chapter is pp. 151-172.
ReplyDelete2. Cath lab does not need to be activated based on the first, even with a positive troponin. There is no sign of persistent occlusion on that ECG; persistent occlusion is the indication for immediate PCI.
3. Yes, inverted T waves on leads overlying the affected wall are analogous to upright T waves on leads distant from the affected wall (i.e. anterior leads for posterior STEMI)
I just read your section on the first book (a great book indeed), and my first question is answered.
ReplyDeleteThanks for 2 and 3 too.
Iatrophobic,
ReplyDeleteHave you read "the ECG in Acute MI" or "Critical Decisions...."?
Feel free to write a book review on Amazon!
Dr. Smith
Dear Dr. Smith,
ReplyDeleteThank you so much for this excellent example. I am a third year medical student and I was wondering if there are any accepted criteria for psuedonormalization in terms of size or character when one sees what may be psuedonormalization.
Thank you!
I could only say that the T-wave will normalize without re-occlusion over weeks to months, but if it becomes upright within hours to days, then it is true pseudonormalization until proven otherwise.
ReplyDeleteDear Dr. Smith
ReplyDeleteI'm a cardiology fellow in Spain. I have had recently a patient with very similar ECG findings related to a subacute complete oclussion of a stent placed in proximal LAD. T waves pseudonormalization was the only remarkable ECG sign. Could you please recommend me any reference related to this issue??.
Thanks very much for your attention.
Have you seen the other cases I have here? See here:
Deletehttp://hqmeded-ecg.blogspot.com/2009/12/pseudonormalization-of-t-waves-coronary.html#comment-form
Pepita,
ReplyDeleteThere is very little literature on this.
A google scholar search came up with a few:
http://scholar.google.com/scholar?start=20&q=pseudonormalization+of+T-waves+reocclusion&hl=en&as_sdt=0,24
I am very interested in your case and would like to see it, maybe post it here. I would of course credit you with the case.
Email me at: dr.smiths.ecg.blog@gmail.com
Steve Smith
hi,
ReplyDeletewhat if the T waves inversion remain inverted even after several years post MI s/p stent and become upright when the pt has new onset of chest pain? Would the upright T wave now after several years of inverted become be a concern?
thanks
True pseudonormalization happens in the acute or subacute phase only. Maybe first 2 weeks. After that, the T-wave usually normalizes as part of the natural history of the NonSTEMI.
DeleteSteve Smith
I noticed on the first 2 ECG's that V3 (which is usually the isoelectric lead, as far as I know) was not isoelectric, V2 was and there were prominent, tall R waves. Yet after stenting, V3 became the isoelectric lead with normalized R waves in the anterior leads like normal. How does that relate to this case?
ReplyDelete