
A middle aged male with history of STEMI and stents presented with one hour of chest pain.
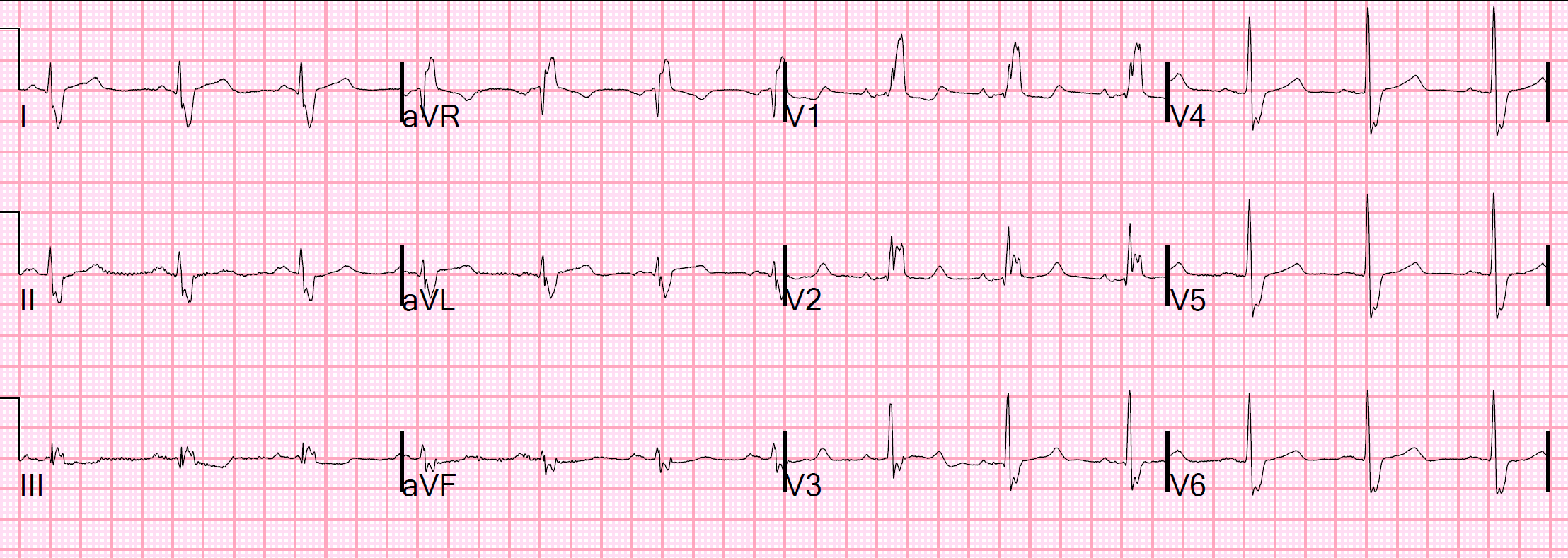
Here is his ED ECG:

There was a previous ECG from 2.5 years ago:

Outcome:
The first high sensitivity troponin was 8 ng/L (normal).
The cath lab was activated by the emergency physicians and the patient went to Angiogram:
Large coronaries with some slow flow. TIMI-2 flow in LAD and First Diagonal.
Mild Plaque no angiographically significant obstructive coronary artery disease.
Cardiology note:
Coronary angiography did not show a definite culprit lesion to explain his acute chest pain. No intervention was performed. His chest pain resolved near the end of the procedure. Nitro drip was titrated to pain control and metoprolol 12.5 mg Q6H was initiated. The patient's pain resolved and the nitro drip was weaned off. Given non-occlusive findings on angiogram, differential for his symptoms includes but is not limited to vasospasm, autolysed thrombus after plaque rupture, and myocarditis vs endocarditis.
Peak troponin was 16,123 ng/L (consistent with STEMI/OMI or with myocarditis)
There was TIMI-3 flow in all arteries, without any culprit found. But pain resolved near end of procedure and next troponin was 16,000!! This is MINOCA (MI with NonObstructive Coronary Arteries.).
It was treated as if it was ACS with medical therapy.
The angiogram is NOT the gold standard for determining occlusion at the time of recording of the ECG. This would be classified as MINOCA
ECG after angiogram:
Formal echocardiogram:
Normal left ventricle.
Left ventricular hypertrophy concentric .
Normal estimated left ventricular ejection fraction .
Regional wall motion abnormality-distal septum anterior possible.
They did a CT coronary angiogram to better elucidate any plaque and to get a better look at wall motion.
There is a small wall motion abnormality in the mid anterior wall of the left ventricle.
Details of CT Coronary angiogram:
LAD: Proximal LAD is a large vessel, measuring up to 10 mm in diameter, with diffuse noncalcified wall thickening. Small caliber first diagonal.
There is a large second diagonal branch with extensive wall thickening, and mild osteal stenosis. The distal LAD is a small vessel.
Circumflex: Large vessel proximally with diffuse wall thickening. There is focal severe stenosis of the mid AV groove circumflex, patent distally.
Prominent first obtuse marginal with questionable ostial stenosis.
Posterolateral branches are patent.
Right coronary artery: Large vessel proximally with diffuse wall thickening. The acute marginal, and posterior descending arteries are patent.
Thus, the CTCA showed diffuse coronary wall thickening.
In other words, because an angiogram is a "lumenogram," the angiogram could not demonstrate the extraluminal plaque which is present. Only the CT could see these plaques, one of which is believed to be the source of the thrombus and which caused the OMI and then lysed (disappeared!). leaving only some slow flow.
Intravascular ultrasound (IVUS) is also used to find extraluminal plaque. See this case: Wellens' syndrome, no culprit, what happened?
Two patients with RBBB

This next ECG comes from this post:
PseudoSTEMI and True ST elevation in Right Bundle Branch Block (RBBB). Don't miss case 4 at the bottom.

Here is the same ECG with lines drawn at the end of the QRS:

Learning Points:
1. In RBBB, ST Elevation in I and aVL, with reciprocal ST depression in inferior leads, may be baseline/non-ischemic! However, you must assume the worst until proven otherwise.
2. The angiogram is not the final arbiter of OMI. In this case, there was OMI, the ECG manifested OMI, but the artery was open at the time of angiogram and the culprit could not be found. It could only be inferred from the diffuse extraluminal coronary disease found on CT
3. Bottom line: the ECG at the top does indeed represent RBBB with Occlusion MI in I, aVL
MY Comment by KEN GRAUER, MD (4/11/2022):
===================================
- KEY Historical Point: The middle-aged man in today's case had a history of prior STEMI with stents placed. He presented to the ED with new chest pain of ~1 hour duration.
- As per Dr. Smith — ECG #1 shows sinus rhythm with complete RBBB. While true that leads I and aVL sometimes mislead, in that they may show some ST elevation in patients with RBBB but not infarction. That said — I thought the amount of J-point ST elevation in these 2 high-lateral leads was excessive, compared to the lesser amounts I was used to seeing in RBBB patients without acute MI (BLUE arrows in leads I, aVL in ECG #1).
- Equally excessive reciprocal ST-T wave changes are present in leads III and aVF.
- Normally with "simple" RBBB — there is at least some degree of ST-T depression in 2 or more anterior leads. I saw less than the "amount" of ST-T depression that I would normally expect in lead V1 of ECG #1 — with if anything, slight J-point ST elevation in lead V2 (BLUE arrow in this lead). The upright T wave seen already in lead V2 is definitely not an expected finding with simple RBBB.
- A fairly large Q wave is seen in lead V1. Tiny-but-present q waves (that might be relevant) are present in leads V2 and V3.
- Lead V3 in ECG #1 shows a slight amount of "scooped" ST depression.
- Leads V4 and V5 show definite straightening of their ST segments, with a hint of ST depression.
- Lead V6 is uninterpretable — which is unfortunate given the abnormal findings in neighboring leads.
- Did YOU Note the marked fragmentation (notching) of QRS complexes in multiple leads?
- BOTTOM LINE for ECG #1: I could not be certain what might be "new" vs "old" in ECG #1. That said — this definitely is not a simple RBBB tracing. The marked fragmentation tells us (as does this patient's history) — that there is underlying coronary disease. The other abnormal ST-T wave findings described above have to be assumed acute until proven otherwise — and I also thought that this patient might have multi-vessel disease.
-USE%20copy.png) |
| Figure-1: I've put the 3 ECGs from the patient in today's case together — and I've labeled the subtle-but-real ECG findings (See text). |
- RED arrows in leads I, aVL and III of ECG #2 confirm that the excessive amount of J-point elevation or depression in these leads in ECG #1 was indeed a new finding.
- Subtle-but-real differences were also present in each of the labeled leads. The scooped ST depression that was seen in leads aVF and V3 of ECG #1 was not present in the prior tracing. And the ST segment in ECG #2 showed a gentle upsloping (curved RED lines) compared to the BLUE line straightening in leads V4, V5 of ECG #1.
- Multiple fragmented leads were present on the prior tracing. However, the Q waves in anterior leads was not.
- BOTTOM LINE: The prior tracing from 2.5 years earlier (ECG #2) was also not a "simple" RBBB ECG — because there was already marked fragmentation of multiple QRS complexes — and — the T wave in lead V2 was already upright. But many of the other subtle ST-T wave abnormalities noted above for ECG #1 were new and consistent with the markedly elevated serum Troponin value.
- Take-Home Message: Careful comparison of prior and serial ECGs, correlated to clinical events can be tremendously insightful — and, in conjunction with results of other testing — may strongly support a presumed diagnosis of acute OMI despite non-obstructed coronary arteries on cath.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.