
Written by Clare Gunn MD, peer reviewed by Smith, Meyers, Bracey
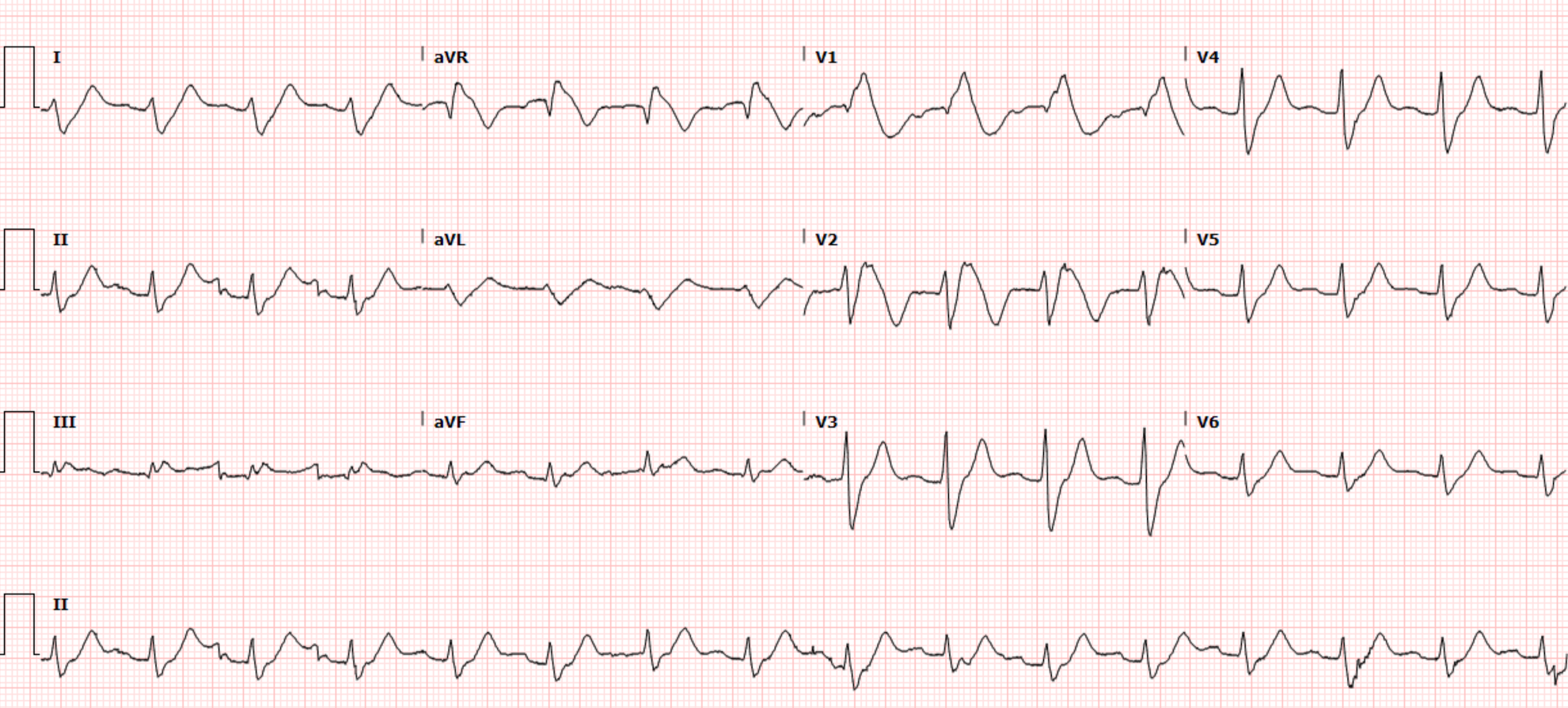
A 74-year-old female presented to the ER after a trip and fall (unclear if purely mechanical or due to possible unsteadiness) causing her to cut her leg. Due to chronic anticoagulation for atrial fibrillation, she could not stop the bleeding, so she came the ED. On arrival she is found to be hypoxemic requiring four liters of oxygen via nasal cannula. While getting her leg wound repaired, the patient was also evaluated for hypoxemia and tachycardia and was found to have this ECG:
 |
| What do you think? |
 |
| RBBB at baseline. |
EKG interpretation:
Wide complex regular tachydysrhythmia at around 100 bpm
Very wide and bizarre QRS morphology, very difficult to precisely figure out where the QRS ends, but my guess is that the QRS is about 200 msec in width. It does have a RBBB configuration, with a large upright QRS in V1 and a wide S-wave in V6. This suggests that the known baseline RBBB is further distorted by additional pathology. Computer QRS duration was 189 msec.
For this highly bizarre QRS complex, there are similarly bizarre ST segments and T waves. In some leads there is a sine wave appearance.
The rhythm is not totally clear. The differential includes sinus or accelerated junctional rhythm with massive conduction aberrancy. I do not think there is any definite atrial activity that can be seen. VT by definition cannot be 100 bpm or lower, and is only very rarely as slow as 120 bpm.
I texted this ECG to Dr. Smith without any clinical information and without the previous ECG, and he immediately texted back: "HyperK, or Na channel blocker such as TCA or Flecainide."
The most common cause of a QRS this wide and weird would of course be hyperkalemia. But the second most common cause is sodium channel blocker toxicity, which can be seen in many tox syndromes, for example tricyclic antidepressants, diphenhydramine, and drugs intentionally designed to block Na channels such as flecainide, procainamide, etc. Conduction abnormalities due to hyperkalemia or drug toxicity will often cause ST elevation (as in V1-V3 in this case) which the computer may report as "STEMI." It is necessary to instantly recognize that the bizarre features of the QRS complex, including the STE, are related to a metabolic process and not OMI in order to avoid early diagnostic closure.
Impression:
This ECG is highly concerning for hyperkalemia or sodium channel
blocker toxicity. Since the heart rate is only barely above 100 bpm, the exact rhythm in this case is not as important as understanding that the QRS is acutely widened by toxicologic/metabolic causes.
Case continued:
The ED provider was appropriately concerned for hyperkalemia first, and promptly gave the patient 2 grams of calcium gluconate with minimal change in her ECG (Meyers side note: 2 grams of calcium gluconate may not be enough calcium to see obvious QRS narrowing in all cases of hyperK! More will not hurt, and in some cases much more will be required before proving that it isn't hyperK). When her lab work resulted, her potassium was only 5.3 but she was noted to have a newly elevated creatinine at 2.2. Further review of the EMR demonstrated that the patient was prescribed flecainide for atrial fibrillation and had recently had her dose increased significantly. Toxicology and cardiology were consulted, and the patient was determined to have flecainide toxicity likely related to her acute kidney injury and increased dose. She was given several boluses and a drip of sodium bicarbonate, but did not seem to immediately respond. She was admitted to the ICU for close monitoring.
The ICU notes describe a sudden change in her rhythm, in which there was still wide complex regular tachycardia, but the ventricular rate rose to 140 bpm. They interpreted this as likely ventricular tachycardia, did not record an ECG of it, and decided to synchronized cardiovert. Following cardioversion attempt, they state that the heart rate went back down to around 100-110 bpm.
Her QRS slowly narrowed over the course of several days.
Here is her ECG approximately one day later:
Day 2:


She was ultimately discharged to rehab with no further anti-arrhythmic therapy. Below is her ECG one week later:
 |
| Computer QRS duration = 138 msec |
Learning points
QRS widening is the result of either (or both) physical or chemical aberrancy of the action potential propagation, compared to normal using a normal Purkinje conduction system. Physical aberrancy includes bundle branch blocks, nonspecific intraventricular conduction delays, cardiomyopathies, bypassing of the conduction system such as paced rhythm, etc. "Chemical" aberrancy involves a slower speed of action potential propagation, such as hyperkalemia or sodium channel blockade. Every wide QRS complex must have at least one of these components to explain why it is wide.
Any RBBB that has a QRS duration longer than 170 ms is likely due to an additional QRS lengthening pathology:
Is This a Simple Right Bundle Branch Block?
Flecainide, the culprit drug in this case, is a Class 1C antiarrhythmic that functions by blocking the fast inward sodium channels that are open during phase zero depolarization of the cardiac myocytes and His-Perkinje system. This results in prolonged depolarization and slowed conduction. Flecainide also acts on inward potassium channels affecting the refractory period of cardiac cells making it well suited for its roll in preventing tachydysrhythmias like atrial fibrillation and other SVT’s.
Flecainide is renally cleared and acute or chronic kidney injury can increase plasma levels of the drug. Toxicity is often recognized in patients due to their bizarre ECGs. Patients will have wide QRS complexes, prolonged PR intervals and prolonged QT’s. Goals of treatment of flecainide toxicity include the management of airway, breathing, and circulation in critically ill patients, avoiding further blockade of sodium channels and prevention of arrhythmic events. Early and aggressive administration of sodium bicarb can help overcome sodium channel blockade and lipid emulsion has been used in cases of severe overdose. There does not appear to be a role for hemodialysis at this point. Early involvement of a poison center or toxicologist is recommended for severe cases.
Having a broad differential for any ECG that is handed to you is
important. Treating this patient for assumed hyperkalemia is safe and would
have been lifesaving if the bizarre morphology above had been caused by
elevated potassium levels but don’t forget to check your patient’s medication
list for medications like Flecainide that cause sodium channel blockade as they
can also produce strange QRS morphologies at therapeutic and especially in
toxic doses.
References
Smith A, Gerasimon G. An electrocardiographic series of
flecainide toxicity. Indian Pacing Electrophysiol J. 2019 Mar-Apr;19(2):75-78.
doi: 10.1016/j.ipej.2018.11.012. Epub 2018 Nov 28. PMID: 30502382; PMCID:
PMC6450827.
Mazer-Amirshahi M, & Nelson L.S. (2019).
Antidysrhythmics. Nelson L.S., & Howland M, & Lewin N.A., &
Smith S.W., & Goldfrank L.R., & Hoffman R.S.(Eds.), Goldfrank's
Toxicologic Emergencies, 11e. McGraw Hill. https://accessemergencymedicine-mhmedical-com.libproxy.lib.unc.edu/content.aspx?bookid=2569§ionid=210273423
Joshua M. Newson,
Cynthia D. Santos, Bradford L. Walters, Brett R. Todd,
The Case of
Flecainide Toxicity: What to Look for and How to Treat,
The Journal of
Emergency Medicine,Volume 59, Issue 2, 2020, Pages e43-e47,
ISSN 0736-4679,
https://doi.org/10.1016/j.jemermed.2020.04.052.
(https://www.sciencedirect.com/science/article/pii/S0736467920303905)
Other cases from this blog:
Here, Flecainide toxicity mimics anterior OMI:
Right Bundle Branch Block with New Anterior ST elevation

Here, Flecainide toxicity in the setting of ventricular paced rhythm mimics hyperK:
Weakness and Dyspnea with a Sine Wave. It's not what you think!

Finally, a fascinating case of the odd aspect of"use dependence" with flecainide toxicity: it's effect on the QRS is often dependent on the heart rate.
Note how the QRS gets wider when the HR gets higher:

No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.