
Wide-complex tachycardia: VT or aberrant, or "other?"
This case is contributed by Brooks Walsh, an EM physician and ECG expert from Connecticut.
The case
An older woman presented to the ED with dyspnea, diaphoresis, and chest pressure.
The patient had a history of paroxysmal atrial fibrillation and several cardioversions. She had a normal EF, and no significant CAD, and was taking flecainide to suppress the AF.
The initial ECG:
 |
The rhythm is regular at 150, and the QRS is markedly wide.
There are small deflections that may be P waves,
but they are not dissociated from the ventricular complexes.
|
A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. And indeed the QRS morphology strongly supported VT (e.g. the R-S interval is greater than 60 ms, and aVR had a broad initial R). Flecainide is well-known to precipitate VT.
However, we considered a supraventricular cause. Sinus tachycardia with aberrancy was unlikely as the rate was consistently 150 bpm, without spontaneous variation.
Instead, the rate of 150, plus the history of AF, suggested atrial flutter. A close inspection of lead II showed P or flutter waves at a rate of about 300 bpm, also supporting atrial flutter.
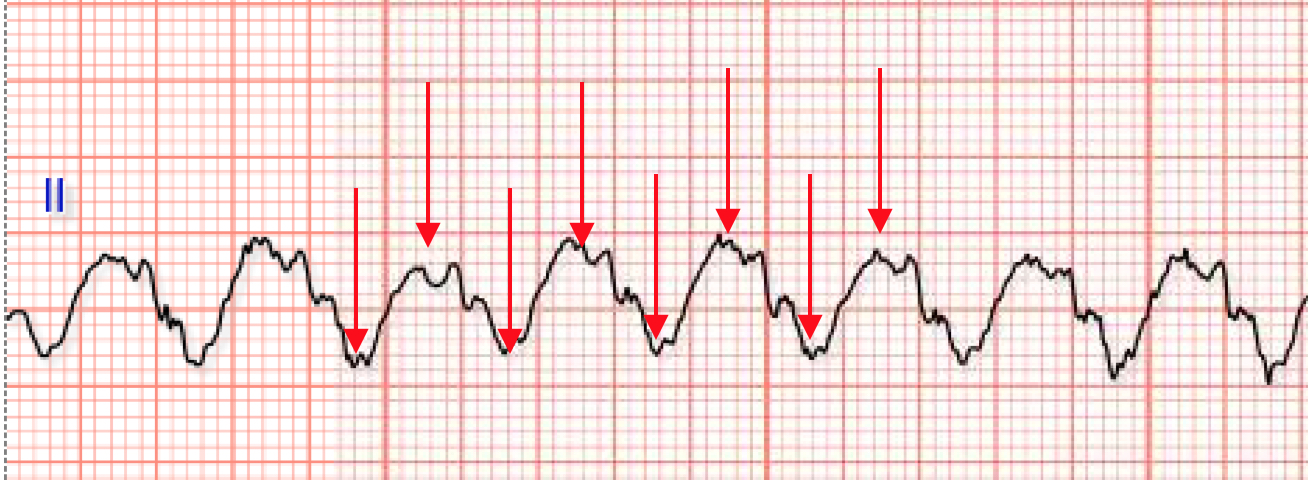 |
| There appear to be flutter waves at a rate of 300. Are they? Such a fast flutter rate in the presence of flecainide is unusual, as flecainide usually slows the rate of atrial conduction (such a slow rate can result in 1:1 conduction) |
A test dose of adenosine was given to check for flutter waves. A rapid push of 12 mg generated the full symptomatic response (gasping, CP, apprehension), but no budge on the rate. This is some strong evidence that it is NOT supraventricular, but indeed VT.
Further diagnostic maneuvers were deferred. Synchronized cardioversion at 360J biphasic produced:
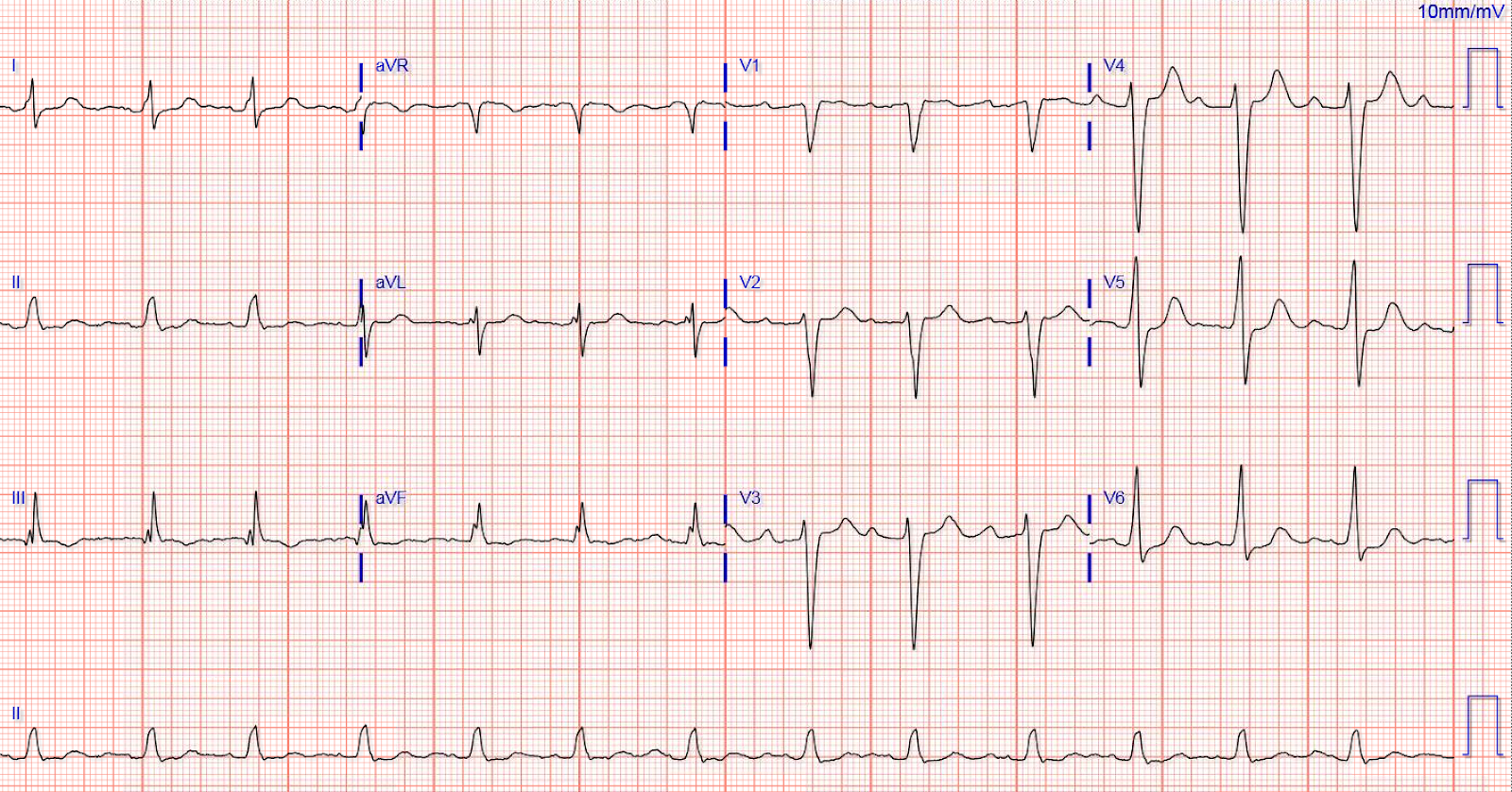
Sinus rhythm with a prolonged PR, but a narrow QRS.
So was this VT after all?
Usually interpretation of the wide-complex tachycardia is framed as deciding between VT, or a supraventricular rhythm with aberrancy. However, a wide complex rhythm can be produced by other problems, and flecainide toxicity is one of those.
A few key facts about using flecainide for AF:
- It can provoke VT, especially in patients with prior MI.
- It is easy to accidentally overdose.
- Toxicity can produce a "bizarre" wide QRS, a long PR, and a wide tall terminal R in aVR.
- Flecainide is use-dependent; it has greater effect at high heart rates.
- Accordingly, signs of toxicity (wide QRS) are greater at higher rates.
- Flecainide encourages new atrial flutter. Atrial flutter is particularly dangerous in patients on flecainide because is slows the atrial flutter rate to a point where 1:1 conduction is possible (e.g., 200), resulting in a dangerously fast ventricular rate. AV-nodal blockers are usually given to all such patients in order guard against this.
The use-dependence of flecainide in the setting of modest toxicity was nicely illustrated on an ECG from the next day (see below). The AF started as a narrow complex, but transitioned to a wide complex as the rate increased in beats #13-18. The morphology of the wide beats was inconsistent with rate-related BBB.
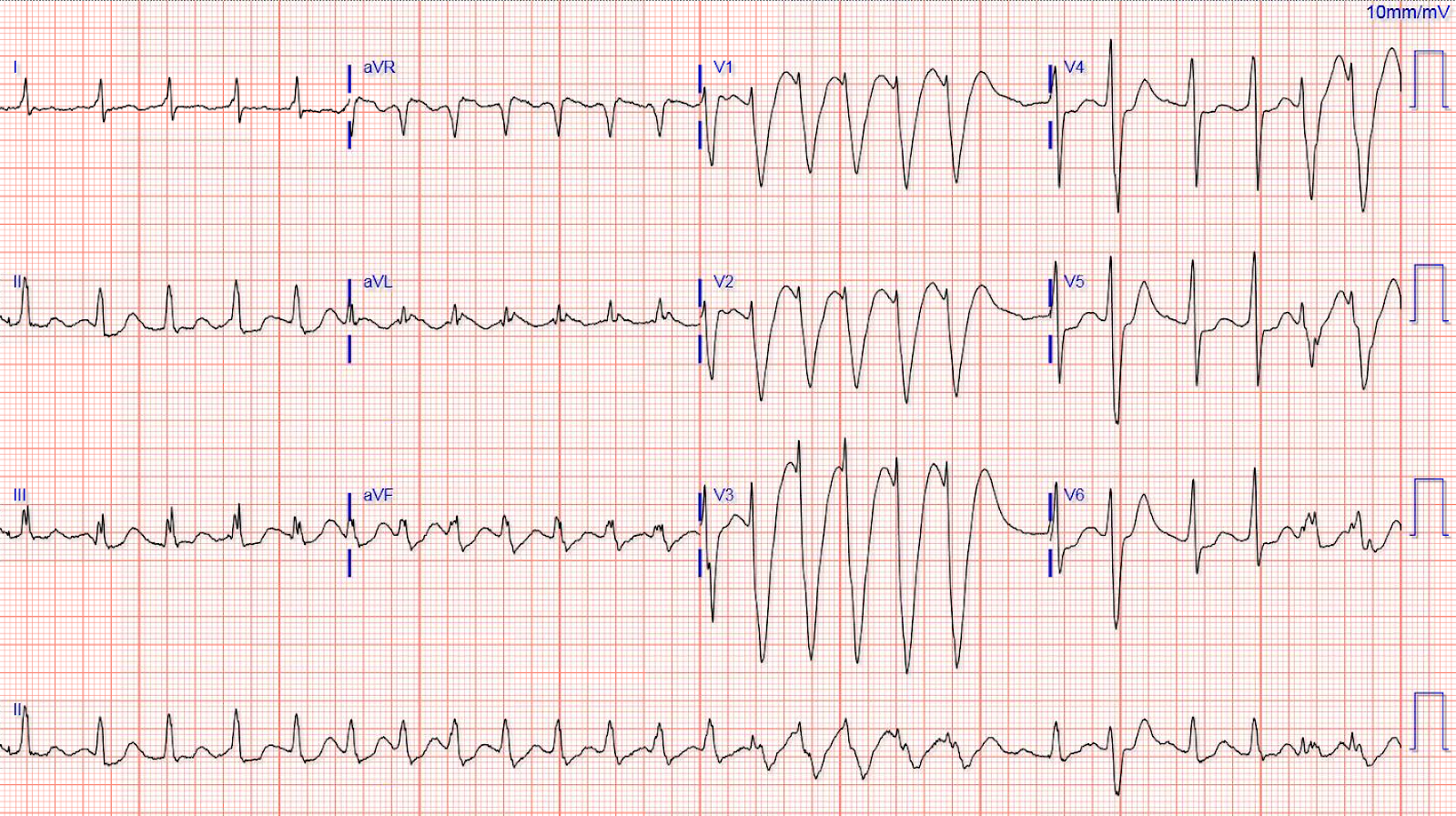
Note that the QRS in beats 13-18 shows a slurred S wave downslope in V1
that would be diagnostic for VT under Brugada criteria.
However, the widening is coincident with the rate increase, typical for the use-dependent
character of flecainide toxicity.
This ECG supports that the wide-complex tachycardia seen in the ED was 2:1 atrial flutter with QRS widening due to use-dependent toxicity, and not due to VT.
Note of Caution!
While a number of EPs have agreed that the initial rhythm was most likely atrial flutter, at least one strongly believed it was VT.
Management of similar rhythms must always take this ambiguity into account!
(For example, do not give a calcium-channel blocker if VT is even a slight consideration.)
Follow-up:
Further discussion with the patient revealed that they had misunderstood the flecainide dosing, and had basically tripled their dose! Additionally, her beta-blocker dose had been decreased because of bradycardia, further predisposing her to atrial flutter. During hospital admission she had a variety of atrial arrhythmias, which eventually resolved, likely due to her decreasing flecainide level.
Flecainide and the ECG: Key Takeaways
- A wide-complex tachycardia in a patient taking flecainide will often be VT, of course!
- However, if the ventricular rate is 150, consider new atrial flutter with 2:1 AV conduction, and QRS widening due to toxicity.
- Atrial flutter can present with 1:1 AV conduction in flecainide toxicity, owing to slower atrial conduction. (The flutter/ventricular rate will be around 200 bpm.)
- Lastly, the WCT associated with flecainide toxicity isn’t identified well by algorithms that differentiate VT and SVT with aberrancy (e.g. Brugada, Varecki).
- We still do not know for certain whether this was atrial flutter at a rate of 300 with 2:1 conduction, or if it was VT.
- Smith comment: I think the strongest evidence that it was VT is that flutter in the presence of flecainide would be very unlikely to have an atrial rate of 300.
===================================
My Comment, by KEN GRAUER, MD (12/16/2018):
===================================
I love cases from Brooks Walsh — as they are always superb learning experiences based on his “being there” on the front line in the ED, with the patient in front of him. I found this case especially intriguing — because even the EP cardiologists in on the case did not all agree. So, while the “Bottom LINE” is that we do not have a definitive answer — in the interest of academic discussion, I’ll present my rationale for why I believe the initial ECG shows AFlutter (and not VT), in this patient with Flecainide toxicity.
- For clarity — I’ve put the 1st and 3rd ECGs in this case together (Figure-1) — and have labeled what for me constitute KEY findings.
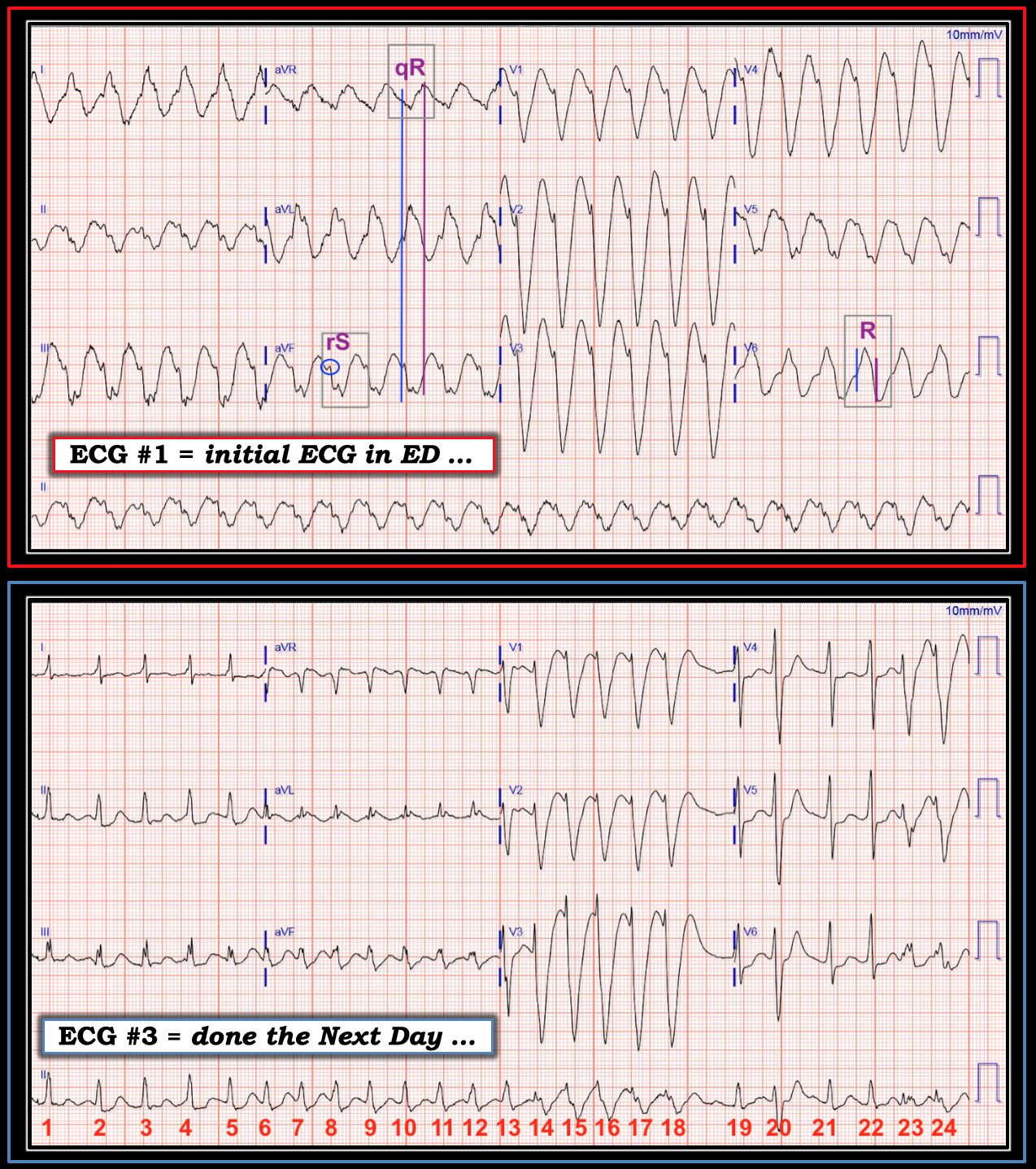 |
| Figure-1: TOP — ECG #1 ( = the initial ECG performed in the ED). BOTTOM — ECG #3 in this case (done the next day). Key findings are labeled. |
==========================
MY THOUGHTS on this CASE:
As per Dr. Walsh — the initial ECG in the ED shows a regular WCT (= Wide-Complex Tachycardia) at ~150/minute, without sinus P waves. Statistically, in an emergency setting — VT is far more likely than SVT (ie, >90% probability) when a patient with heart disease presents in a regular WCT without sinus P waves. Therefore (as emphasized by Dr. Walsh) — VT should always be assumed until proven otherwise.
- BUT — this patient was known to be on Flecainide for treatment of PAF (Paroxysmal AFib). And, among potential manifestations of Flecainide Toxicity are: i) QRS widening which may be marked, often with bizarre QRS morphology; ii) Slowing of conduction in atrial and ventricular tissue, as well as in the His-Purkinje system; iii) VT, as a proarrhythmic effect; and, iv) facilitating conversion of AFib to AFlutter, as another proarrhythmic effect.
COMMENT: Awareness of these potential manifestations of Flecainide Toxicity should alter our use of traditional assessment factors for distinguishing between SVT vs VT. For example:
- Statistical likelihood that the regular WCT in ECG #1 might be AFlutter (instead of VT) is greatly increased in a patient with AFib who is taking Flecainide. In such a patient, we need to significantly adjust downward the statistical likelihood that a regular WCT without P waves is VT.
- If AFlutter does develop as Flecainide-induced proarrhythmia — we should expect unusual QRS morphology with marked QRS widening. As a result — use of traditional QRS morphology characteristics will usually not be helpful in distinguishing between VT vs SVT, because the QRS complex in Flecainide-induced AFlutter is unlikely to resemble any form of conduction defect (CLICK HERE — for my approach using QRS morphology with WCT).
- Because of Flecainide’s adverse effect on conduction through atrial, ventricular and His-Purkinje tissue — the usual diagnostic and therapeutic effects of antiarrhythmic agents may be much less effective (if they are effective at all). This probably accounts for the refractoriness of Flecainide-induced proarrhythmia to antiarrhythmic treatment. In this particular case — it may account for diagnostic failure of Adenosine to slow AV conduction in a patient with AFlutter.
==========================
Editorial COMMENT — More of a “confession” than a comment — I fully acknowledge spending close to an hour with calipers, trying to prove that I was seeing 2:1 AV conduction in ECG #1. Suffice it to say that I failed to do so. The inferior leads (and especially the long lead II rhythm strip) — to me were most suggestive of 2:1 Flutter — but ECG #1 is marred by baseline artifact and, no matter how hard I tried, I could not march out consistently precise 2:1 activity as should be possible if the rhythm was 2:1 AFlutter.
- Perhaps flutter waves are hidden within artifact, within ST-T waves, and by the wide, bizarre QRS complexes?
- Perhaps the reason the rhythm in ECG #1 is regular, but without 2:1 flutter waves — is that we are seeing 1:1 AFlutter, due to marked atrial slowing from Flecainide toxicity?
==========================
Why I Think ECG #1 is Not VT: The argument is made above by Dr. Walsh that QRS morphology in this case strongly supports VT as the rhythm in ECG #1. I respectfully disagree.
- Measurements regarding slow initial depolarization, and delay until peak negativity are irrelevant for distinguishing SVT from VT in light of Flecainide toxicity. That’s because both VT and Flecainide-induced AFlutter demonstrate delay in ventricular conduction.
- The initial deflection in lead aVR is not positive, but negative (See vertical BLUE line showing that initial negativity in aVR corresponds with onset of the QRS complex in simultaneously-obtained leads aVL and aVF). This is far less predictive of VT than if the QRS complex in aVR was completely positive.
- Extreme axis deviation in the frontal plane is not present — because a small-but-definitely-present initial r wave is seen in all 3 inferior leads (See within the BLUE circle in lead aVF). Specificity of frontal plane axis deviation is unacceptably poor as a sign for distinguishing SVT from VT when the QRS complex is not all negative in either lead I or in lead aVF.
- QRS morphology in the chest leads is consistent with a supraventricular etiology — since a monophasic R wave is present in lead V6.
- Finally — I believe a plausible pattern for progressive QRS widening with a rate-related component of aberrant conduction is seen in this patient with Flecainide-induced proarrhythmia.
==========================
COMMENT: The ECG obtained the next day on this patient ( = ECG #3) is telling. The underlying rhythm is AFib (irregularly irregular QRS without P waves).
- Note QRS widening for beats #14-thru-18 in ECG #3. This illustrates the use-dependent phenomenon mentioned earlier by Dr. Walsh (greater effect on QRS widening from Flecainide toxicity at faster heart rates). That this 5-beat run is still AFib is suggested by slight-but-real irregularity to caliper measurement of the R-R interval during these 5 beats (the rhythm in ECG #1 was virtually clockwork regular!).
- Note that beat #19 in ECG #3 narrows! This supports a rate-related aberrancy component — because of the brief pause just prior to beat #19.
- The QRS widens a bit in beat #20 — compared to the narrower QRS of neighboring beats #19, 21 and 22. This is again consistent with a rate-related aberrancy component by the Ashman phenomenon (in which aberrancy follows a relative pause).
- Measuring with calipers, the rate then speeds up slightly for beats #23 and 24 — and we once again see QRS widening (ie, rate-related aberrancy) for beats #23 and 24.
- Now look at the long lead II at the bottom of ECG #3 in its entirety. Note how the rate of the underlying AFib begins SLOWER than 150/minute for the first few beats! Thus, the rate for these first few beats is slower than the 150/minute rate seen in ECG #1. That’s why the QRS complex is much narrower (virtually of normal duration) for beats #1-6 in ECG #3.
- As the rate of AFib gradually (and progressively) increases — the QRS progressively widens, until it becomes very wide for beats #14-thru-18.
- For as wide as the QRS is for beats #14-thru-18 (I measure 0.22 second) — the QRS was wider still in ECG #1 (I measure 0.25 second), in which the tachycardia is sustained.
- The QRS was also wide in ECG #2 (I measure 0.12 second) — which was the tracing recorded right after synchronized cardioversion resulted in sinus rhythm. Presumably, the reason the QRS is “only” 0.12 second in ECG #2 (instead of the 0.25 second for the QRS in ECG #1) — is that the rate in sinus rhythm is now much slower.
- Both QRS duration and QRS morphology in the long lead II of ECG #2 — is very similar to QRS duration and QRS morphology in the long lead II of ECG #3 for beats # 5, 6; and 19, 21, 22.
- ALL points in the above bullets are consistent with what I’d expect in a patient with QRS widening from Flecainide toxicity + a rate-related component of aberrant conduction. Rate-related relationships are not perfect (they never are with rate-related aberrancy — CLICK HERE) — but the overall “theme” of what we see in this case ( = in My Opinion) is certainly consistent with this phenomenon.
- Finally — If one “steps back” to attempt an overall perspective of QRS morphology in multiple leads on these 3 tracings as heart rate increases and the QRS widens (ie, sequentially looking at the less wide QRS in sinus rhythm with ECG #2 — then the changing rates of the AFib tracing in ECG #3 — and then the widest QRS in ECG #1) — I see elements of similarity in QRS morphology in many leads, as I might expect from toxicity-induced QRS widening with rate-related changes. I just would not expect the above findings if ECG #1 was VT …
Would there be value in placing the m-mode cursor through the right atrium on a subcostal ECHO view, to count the atrial rate? Would this change treatment at all?
ReplyDeleteGood idea. That might work.
DeleteI would judge the chest leads as being concordant negative, so this must be VT (from the anterior-apical ventricular myocardium)
ReplyDeleteLook closely and measure: they are NOT concordant.
Delete