
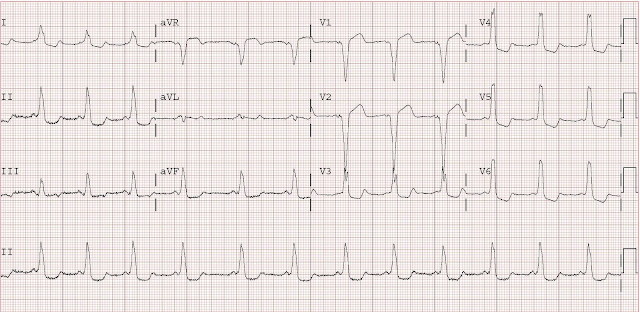
There is striking ST segment elevation in V1 and V2, with ST depression in V3-V6 as well as I, II, and aVF. There is also a wide QRS. One might think this represents acute STEMI, or Bundle branch block with discordant ST segments and suspicously concordant T-waves.
However, closer inspection reveals a very short PR interval and that the wide QRS is due to a slurred upstroke (delta wave).
This is WPW, which is well known to produce pseudoinfarction patterns.
The patient had a positive troponin, underwent cath which showed completely clean coronaries, and then underwent EP testing which revealed that, in atrial fibrillation, he has an R-R interval as short as 220 ms, which is dangerously short. Ablation was planned for a later date.
Wonderful case!
ReplyDeleteI'm curious, however.
Given the widened QRS-T angle, would your modified Sgarbossa's criteria be necessary to diagnose AMI in presence of the WPW pattern?
I know given the relative rarity of such an occurance, this seems purely academic. But still.. your thoughts?
The Sgarbossa criteria, modified or not, cannot be used in this case, because WPW has diverse and unpredictable effects on depolarization and repolarization. The bypass tract location is very heterogeneous from patient to patient, so it manifests differently on every EKG and cannot be predicted.
ReplyDeleteDr. Smith,
ReplyDeleteI'm a cardiology fellow in Chicago and really enjoy your blog. I've learned more from your blog than from most of my attendings about the finer elements of ECG interpretation.
I have an good case for you. I recently got called in for a stemi. The ECG is posted on my blog:
http://blog.thealo.com/thealo/blog/post/EKG-What-is-this.aspx
I'd like to know your thoughts. Feel free to use my ECG for teaching purposes.
My initial thoughts were that this is not an anterior MI by any stretch of the imagination. It didn't have the correct shape of the ST elevations and the reciprocal changes weren't the correct shape and weren't convincing either. I told the attending interventionalist and he agreed with me on what I thought it was, but we had to prove that he didn't have CAD and had to do the cath since the ER already activated the cath lab and everyone was already there.
What are your thoughts on this ECG? I can send you a high resolution scan if you'd like for your books or your blog, if you'd like.
Dr. Alo,
ReplyDeleteThanks for the nice comments. Interesting ECG!
I agree this does not look like a STEMI. It has some of the features of Type II Brugada syndrome: slightly prolonged QRS, downsloping ST segment in V1, saddle configuration in V2. There is also high voltage suggestive of LVH. I do not think you can find an explanation for the chest pain on this ECG.
What was the diagnosis?
Yes, we ended up calling it Type 2 Brugada. We confirmed it with a number of other cardiologists. This is an entity that I have only read about, and never actually seen, so I was fascinated by this.
ReplyDeleteI didn't think of Brugada till after we finished the cath. But immediately when I saw the EKG, I told his mom that he wasn't having an MI, i just did not look like a STEMI ekg.
He may have had some anxiety or chest discomfort and this is just what his EKG will always look like.
The reason these get mistaken for STEMIs is that they have what appears to be "ST elevations" and what appears to be "reciprocal changes" in the correct location (inferior leads), so it can throw people off.
Thanks for the input. If you want a higher resolution image of this for the next edition of your book, let me know.
I purchased your book late last week. I am fascinated and infatuated with your EKG research and analysis. Your book and blog should be required reading for ER/IM and cardiologists everywhere! I frequent your blog more than I am willing to admit, going back over various sections over and over again. I love this blog!