
A young man presented with a gunshot wound to the right chest, with hemo-pneumothorax and hemorrhagic shock.
He got a chest tube and intubation and massive transfusion and stabilized.
CT of chest showed the bullet path through his right lung but nowhere near his heart.
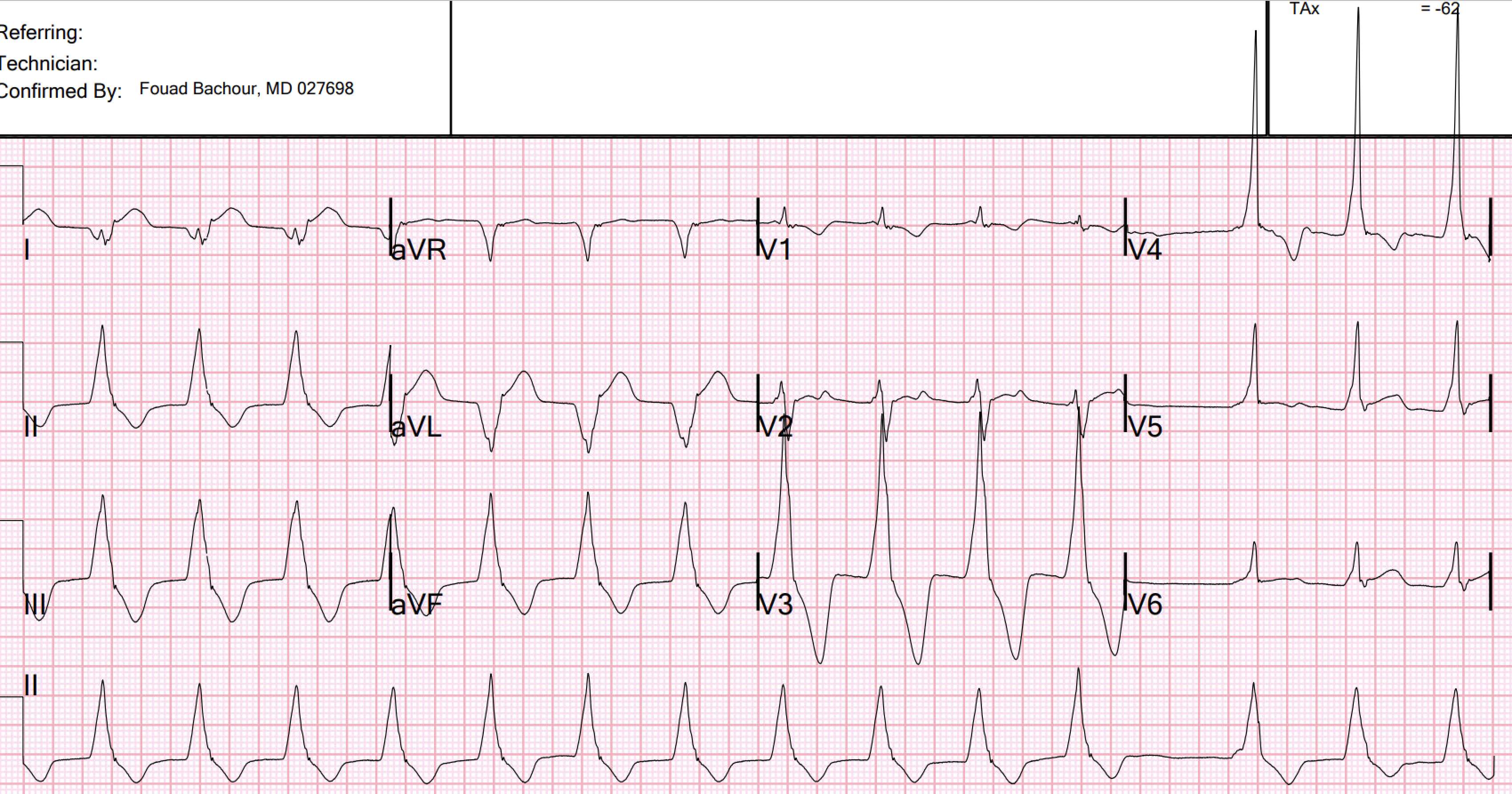
But he did get an EKG:



On that first ECG, I was not entirely certain, since I have never seen nor heard of irregular AIVR, nor can I find a report of it in the literature. But I have seen AIVR in young people with trauma (see case below)
-USE.png) |
| Figure-1: The ECG sent to Ken Grauer (showing some semblance of "group" beating). |
- The QRS is VERY wide — and the very wide Q in lead I (showing marked axis deviation) certainly suggest a ventricular etiology. Lots of leads almost look like delta waves — but I hate to diagnose delta waves when there are no P waves.
- This does NOT seem irregularly irregular enough for AFib … Instead — there is almost “group beating” with “Wenckebach periodicity”. That is, R-R intervals are decreasing within groups — and the pauses (ie, between beats #3-4; 8-9; and 13-14) are less than twice the shortest R-R interval.
- My guess is this is an irregular Accelerated Ventricular Rhythm (which can occur when there is “triggered” activity) — perhaps with Wenckebach conduction out of the ectopic ventricular focus.
- That said — it is not impossible for AFib + complete AV block to manifest Wenckebach conduction out of the AV nodal escape (We used to see this when Dig toxicity was common … ) — but my guess in this case is “triggered” activity irregular AVR …
- In any event — I don’t think I’d try and treat this rhythm given the reasonable ventricular rate (and I’d hope the rhythm improves as the GSW to chest is treated … ).
============================
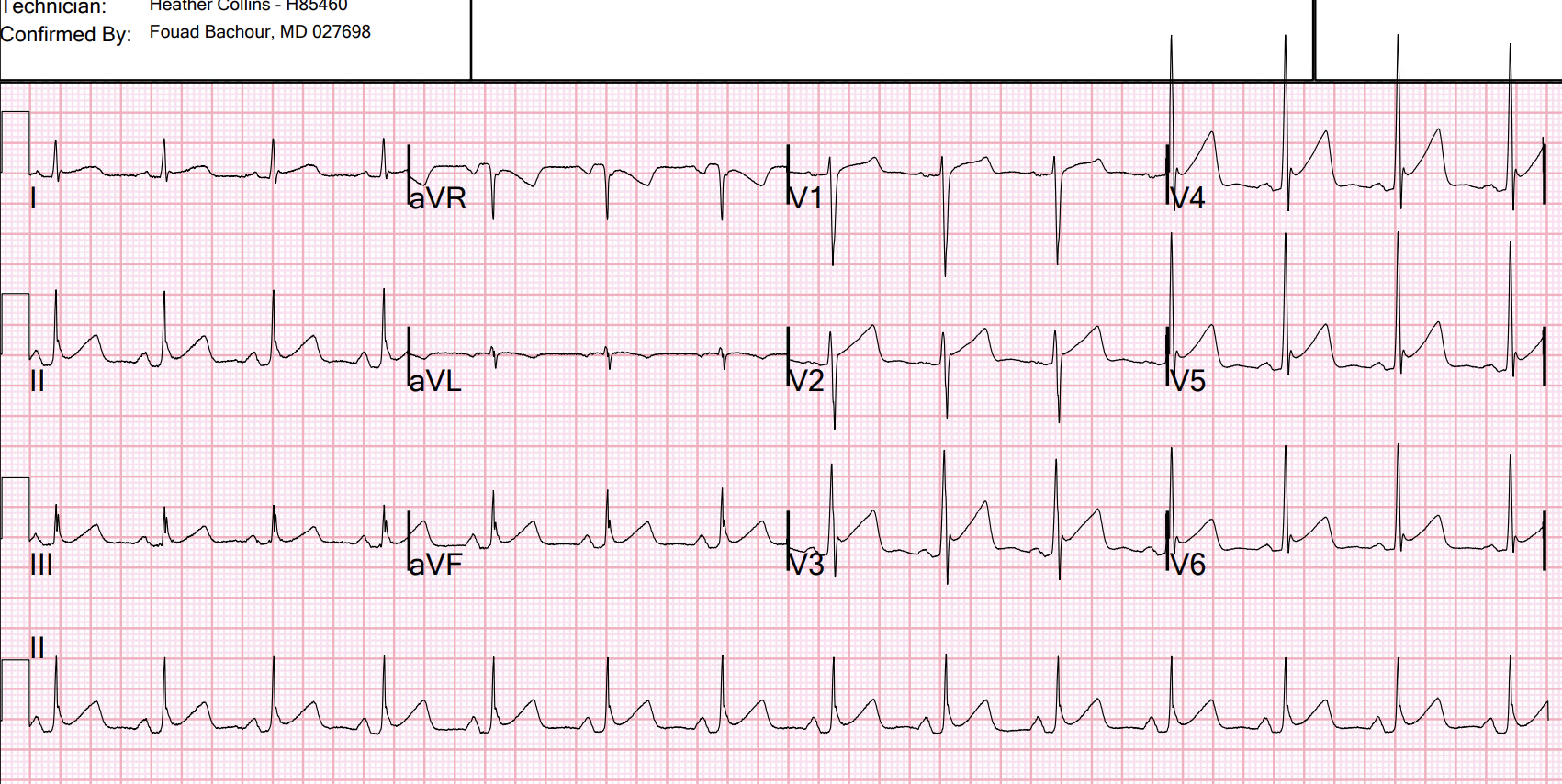
I had a previous case of an adolescent with trauma and chest pain who also had AIVR:
An adolescent with trauma, chest pain, and a wide complex rhythm
From this blog post: "AIVR is NOT common in otherwise healthy children. I’ve attached an article and an abstract (that article is in Japanese unfortunately … ) that do document that you CAN however on occasion find AIVR in otherwise healthy children — and I suppose that IS what we have here. Perhaps the circumstances surrounding the ED visit cause slight acceleration in the ventricular escape rate to allow this all to happen."
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.