
Written by Willy Frick
A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. He said it felt like "someone ripped [his] heart out." Ominous.
While walking into the ED, the patient had an episode of "dizziness" causing him to fall onto his stomach. (Ventricular tachycardia?)

I sent this ECG to Dr. Smith and Dr. Meyers with no context. Dr. Smith immediately replied "Swirl. Proximal LAD." Dr. Meyers agreed.
Here is the PMCardio Queen of Hearts AI ECG Model analysis with explainability:

Not pictured here is the Queen of Hearts confidence level, which was 1.0 (meaning as confident as possible). This ECG is so characteristic of proximal LAD OMI, that even without any clinical context it is hard to imagine that it could ever represent anything else. The most diagnostic findings here are:
- STE and HATW (hyperacute T waves) in V1
- HATW (without accompanying STE) in V2
- Lateral precordial STD (V5-6)
- STE and HATW in aVL
- STD with ischemic down-up T waves in II, III, aVF reciprocal to high lateral injury
- Lead I has subtle STD, probably because the maximal STE vector is so far north
- Leads V3-4 have upsloping STD and HATW, known as de Winter morphology

Although the ischemic signatures are now less pronounced, the ECG still shows LAD OMI. Note the subtle progression of Q wave depth in V2. The Queen of Hearts has no trouble with this.

She remains highly confident for OMI, 0.93. Initial cTnI was 0.007 ng/mL (ref. < 0.022). The patient was admitted. The following morning, the admitting team consulted cardiology. In their consult note, cardiology says the patient has "only minimal chest discomfort," which is another way of saying refractory ischemic chest pain.
Repeat ECG that Saturday night is shown.

This ECG shows progressive infarction with Q waves now much more apparent in V2 and new development of Q waves in V3 even though the patient never manifested anything close to STEMI, and in fact hardly had much STE at all. The cardiology note says to continue medical management, and to proceed with urgent cath if the patient has "recurrent episodes of chest pain unresponsive to meds."

Queen of Hearts calls this OMI with confidence level 0.96, near perfect. Apparently 22.8 ng/mL was the threshold of troponin to be convincing. The patient went for cath at 8 AM Sunday, about 30 hours after he presented.

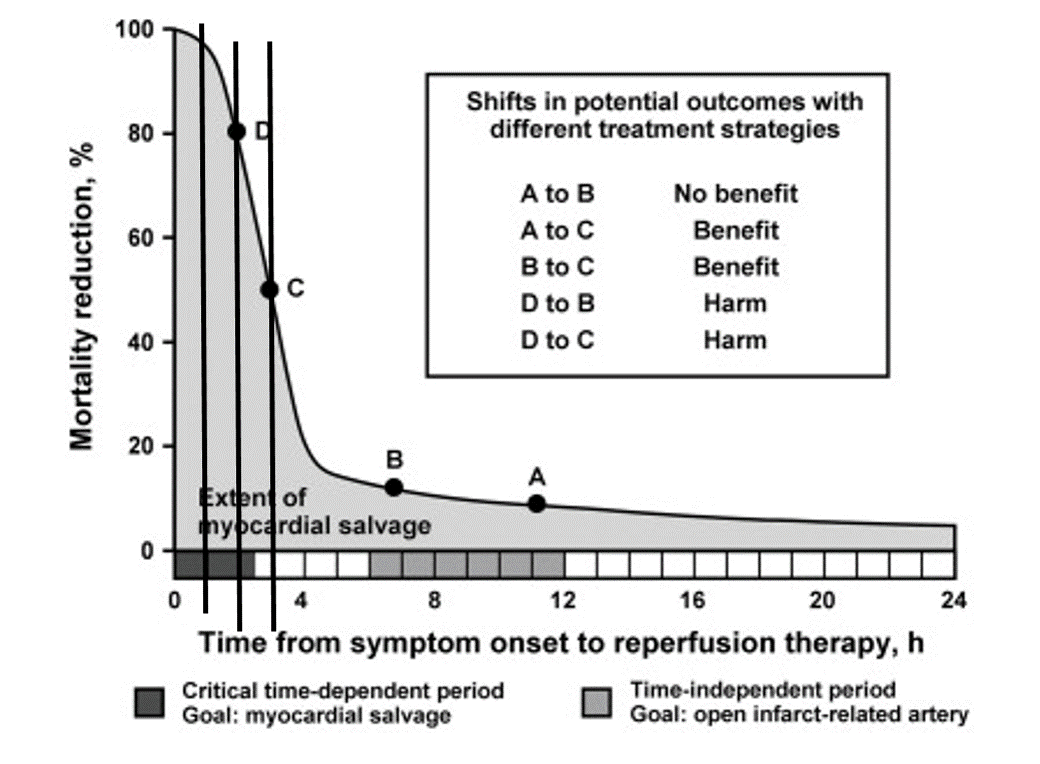
Angiogram showed complete occlusion (TIMI 0) of the proximal LAD, exactly as expected from the precordial swirl. Unfortunately, since most of the salvageable myocardium infarcts within 6 hours (DOI: 10.1001/jama.293.8.979, 10.1161/01.CIR.88.1.296), this PCI was mostly cosmetic.

The patient's heart appears quite laterally oriented, so that the "anterior" wall is really facing more upward. This explains the northward vector of STE.
Case conclusion:
The patient's troponin peaked above the upper limit of quantitation, ">50.000 ng/mL." He developed HFrEF, and after titration to maximally tolerated guideline directed medical therapy, his left ventricular ejection fraction was 25-30% and he was referred for ICD.
Follow up ECG in clinic a few weeks later shows completed infarct.

Discussion:
Why do we let this happen in the era of modern cardiac catheterization and PCI?
Why is a patient allowed to present in the hyperacute phase of LAD OMI and complete his infarct in the hospital under physician care? We could hardly ask for a more obvious clinical history. The patient was quoted in the chart as saying fit felt like someone ripped his heart out.
I am commonly told, and I commonly read in the chart that chest pain is resolved. But often when I talk to the patient myself, they tell me they have residual symptoms. It is not enough for the chest pain to be "much better." The patient has to be rendered asymptomatic for us to have any measure of comfort in delay. It is incumbent upon the clinician to elicit the symptoms, and not to blame the patient as a "poor historian." (The patient is not the historian, they are the source. The CLINICIAN is the historian.)
Smith: Even resolution of symptoms is not enough. There must be resolution of BOTH symptoms and ECG findings (not progression of ECG findings!). Severe ischemia can be present even when the chest pain is gone. See this case.
Cases like these should infuse us all with healthy doses of humility. How confident can we really be that it is safe to delay catheterization?
Another left ventricle sacrificed at the alter of ST elevation.
Learning points:
- 40% of LAD OMI with TIMI-0 flow do NOT meet STEMI criteria (manuscript under consideration at Eur Ht. J Cardiovascular Interventions.--20/53 did not meet STEMI criteria, but all showed OMI diagnosed by both Smith and the Queen of Hearts.
- If the ECG shows OMI, activate the cath lab IMMEDIATELY. Do not wait for troponin.
- We showed that the first troponin is completely negative 25% of the time. So even if you wait for troponin, you often won't make the troponin diagnosis until you wait for another.
- Every hour of waiting kills 25% of the myocardium at risk (see below)
- In the setting of OMI, "minimal chest discomfort" is active ischemic chest pain. Chest pain is not resolved until it is completely gone
- Do not wait to be convinced by troponin
- A patient can complete an anterolateral infarct with TIMI 0 flow and Q waves without ever progressing to obvious STEMI, or even manifesting much STE at all -- see the figure below with serial change across the five ECGs



- In the hope of highlighting some of these oversights — I focus my comments on this patient's clinical presentation in light of findings that should have been appreciated on today's initial ECG.
- For clarity in Figure-1 — I've reproduced and labeled that initial tracing.
- From this patient's clinical presentation alone — the odds of an ongoing acute cardiac event were overwhelming even before looking at the initial ECG (ie, Sudden onset of severe CP that awoke this patient from sleep, feeling like "someone ripped his heart out" — with a near syncopal episode on arrival in the ED). Given this presentation — even modest ECG findings should dictate an exceedingly low threshold for activating the cath lab.
- WHY do I say 12/12 leads are clearly abnormal in this initial tracing? (My specific thoughts on the ECG below).
- Time efficient assessment of this initial ECG given the above history should consist of an immediate phone call to your friendly cardiologist on call — who should be on his/her way to see this patient shortly after receiving that phone call as the cath lab is being activated. Cardiology wasn't consulted until the next day.
- As we have often emphasized in Dr. Smith's ECG Blog — the need for prompt cath in today's case is not in the least dependent on Troponin values. High sensitivity Troponin may initially be normal despite significant infarction. Waiting for a "high Troponin" given today's clinical presentation and initial ECG is indication of not understanding the reality of Troponin fallibility.
- Even though the 2nd Troponin was "not that high" (ie, 1.6 ng/mL) — this is a significant increase from the initial normal Troponin value. Not appreciating that this amount of increase is yet one more reason for activating the cath lab is yet one more critical oversight.
- The ECG was repeated after improvement (but not complete relief) of CP. Although ECG changes were also "improved" — the fact that there was significant change in ST-T wave appearance in association with reduced symptoms is indication of "dynamic" ST-T wave change. Given the clinical history — this is yet one more indication for prompt cardiac cath rather than delay in consulting cardiology until the next morning.
- When cardiology finally saw the patient that next morning — their note said to "Continue medical management, with urgent cath for CP unresponsive to meds". Failure to at least perform cardiac catheterization at that time indicates not having fully reviewed details of this patient's clinical presentation, nor appreciation of "dynamic" ST-T wave changes in association with Troponin rise and only partial relief of CP — all of which combine to confirm an acutely evolving cardiac event.
-labeled-USE.png) |
| In Figure-1 — I've labeled the initial ECG in today's case. |
- My "eye" was immediately drawn to lead aVL (within the RED rectangle). Considering tiny amplitude of the QRS in this lead — there is J-point ST elevation with definite straightening of the ST segment takeoff. Again, considering tiny size of the QRS — the Q wave in this lead is wider and deeper than-it-should-be, and assumed to be significant until proven otherwise.
- In support that the ST-T wave in lead aVL is truly hyperacute — are the marked reciprocal ST-T wave changes in each of the inferior leads (BLUE arrows).
- While the ST-T wave appearance in lead I is more subtle — the ST segment in this lead is clearly flattened, and the T wave appears "bulkier" than would be expected given small amplitude of the R wave.
- With "Swirl" — there is ST elevation in leads V1 and aVR — and reciprocal ST depression in leads V5 and V6.
- I like to focus on the ST-T wave appearance in leads V1 and V6.
- Although 1-2 mm of upsloping ST elevation is commonly (and normally) seen in anterior leads V2 and V3 — most of the time we do not see ST elevation in lead V1 (or if we do — it is minimal!). Therefore — I become immediately suspicious of precordial Swirl whenever there is suggestion of LAD OMI and in addition lead V1 looks different than expected! The distinctly coved (as well as elevated) ST segment in lead V1 of Figure-1 is not a typical picture for the ST segment in this lead.
- Support that this ST-T wave appearance in lead V1 is truly abnormal — is forthcoming from: i) ST segment straightening and a much "fatter" T wave peak than expected in lead V2 considering tiny size of the QRS in this lead; — ii) The small-but-real initial Q wave in lead V2 (PURPLE arrow), that is clearly abnormal because it precedes a small positive r wave deflection in this lead; iii) Abnormal fragmentation of the QRS in lead V1 (within the dotted PURPLE oval); — and, iv) Subtle-but-real ST depression in neighboring lead V3 (BLUE arrow) — whereas there is normally slight, gently upsloping ST elevation (not depression) in lead V3.
- The final part in diagnosing precordial Swirl — is to see reciprocal ST depression at least in lead V6 (if not also in lead V5). What is characteristic of Swirl for this lateral chest lead ST depression — is its more flattened appearance, compared to the downsloping ST segment more typical of LV "strain".
- The remaining 2 leads are lead V4 (which in Figure-1 shows a similar marked and flattened ST segment appearance as we saw in leads V5,V6) — and lead aVR (which shows ST elevation).
- In Summary: Figure-1 is remarkable for showing multiple leads with ST segment flattening and/or depression, in association with ST elevation in lead aVR — consistent with DSI (Diffuse Subendocardial Ischemia). The hyperacute ST-T waves in leads aVL; V1,V2 — with the shelf-like ST depression in leads V5,V6 suggest the cause of this DSI is Precordial "Swirl" from acute proximal LAD occlusion. In this patient with new severe CP — prompt cath is immediately indicated on seeing this initial ECG.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.