
Which patient needs a CT Scan?
Case 1: 20-something woman with chest pain

Case 2: 50-something man with chest pain

Case 1
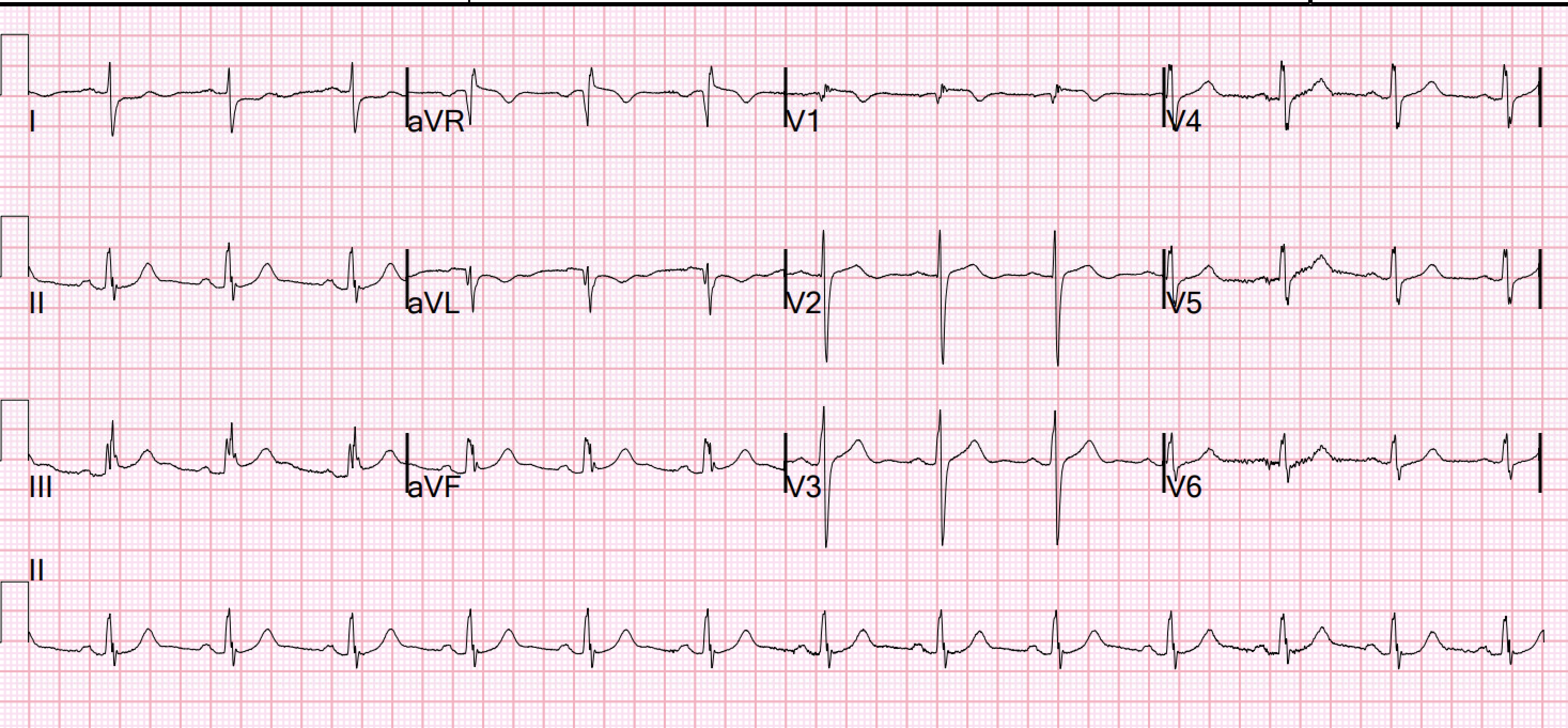
A 20-something yo woman presented in the middle of the night with severe crushing chest pain. It had begun 4 hours before arrival and was initially dull, but became severe and "unbearable" 2 hours prior to arrival. She was a walk-in at triage. She has no SOB and no prior medical history. Her initial BP was 203/124.
She had this ECG recorded:

She was quickly brought to the critical care area and the cath lab was activated.
The blood pressure was 170/100 in the critical care area.
Cardiology wanted a CT of the aorta to rule out dissection, presumably partly due to the very high blood pressure readings, but also because it is hard for people to believe that a 20-something woman could have acute thrombotic coronary artery.
They also recommended a NTG drip, after which she reported complete resolution of pain. No ECG was recorded after pain resolution.
Here is the ECG at 25 minutes:

So a CT scan was done which of course showed a normal aorta. But it also shows a massive area of total ischemia in the LAD territory:
CT shows the infarct


First hs troponin I returned at 256 ng/L.
Angiogram
Door to balloon time was 120 minutes (much too long) because of time taken for a CT.
Coronary angiogram showed 100% mid LAD occlusion for which she received a DES with excellent angiographic result. This was ruptured plaque with thrombus. It was not SCAD (coronary dissection)
A 50-something y.o. male who hasn't doctored in several years presented to the emergency department by ambulance for chief complaint of chest pain.
Here is the prehospital ECG:

Queen of Hearts: "STEMI or STEMI Equivalent detected" (that is, "OMI detected")
The Queen is not wrong very often, so maybe it is an OMI?
History
Patient complains of a 24-hours of chest pain of sudden onset, sharp in nature. Pain started day before and it started on the left side of his face, descended down his neck, and remained mainly in his chest before radiating down his back to his left lower extremity. It persisted through the night (for at least 18 hours), and nothing made the pain better or worse. He had never experienced a similar pain at rest or upon exertion. He reported chest pain 9/10 at the time of evaluation. Denies SOB. Vomited 3 times overnight, not currently feeling nauseous. He denies history of HTN, HLD, DM, smoking. He does not take any medications chronically.
Vital signs were normal.
An ED ECG was recorded:
Initial hs troponin I returned at > 60,000 ng/L
Cardiology was consulted and the cardiology fellow palpated both radial pulses and found that they were very assymetric.
They recommended a CT of the aorta.
Here it is:

Why was the troponin so elevated? And why does the ECG show subtle signs of OMI?
See here that the dissection is very close to the ostium of the RCA. Most dissections which cause coronary ischemia are into the RCA ostium
("ostium" = locations of takeoff of the vessel).

The CT showed extensive type A aortic dissection which starts at the ostium of the RCA and extends all the way to the left iliac artery.



Good Review:
MY Comment, by KEN GRAUER, MD (12/16/2024):
- It is insightful seeing how Aortic CTA (Computed Tomography Angiography) so clearly showed this patient's infarction — thereby confirming the diagnosis of acute MI prior to cardiac catheterization (even though the primary reason for aortic CTA was to rule out aortic dissection).
- It is humbling to realize that bedside Echo revealed normal LV function — whereas formal Echo showed significantly reduced ejection fraction with multiple regional wall motion abnormalities. The accuracy of bedside Echo is clearly a function of operator skill and experience — and at times it may be difficult to exclude the possibility of WMA (Wall Motion Abnormality) from bedside Echo alone.
- The clinical presentation of the patient in Case #1 qualifies as a hypertensive emergency (with the difference between HT "urgency" vs "emergency" being whether or not there is acute end-organ damage — which clearly was present given the large acute infarction).
- Sublingual NTG (nitroglycerin) X3 was no more than minimally effective in relieving this patient's CP (Chest Pain). As a result — IV NTG was started, with complete resolution of the patient's CP (and presumably significant improvement in her marked hypertension)! This raises the question as to how much this patient's hypertensive emergency contributed to her ongoing severe CP prior to initiation of IV NTG — vs — how much her acute MI contributed to her ongoing severe hypertension? (See below).
- And — this patient's initial ECG (that I've reproduced and labeled in Figure-1) shows some interesting findings (See below).
- As noted above — the presence of acute target organ damage in today's case (ie, acute MI) in association with marked sustained hypertension (this patient's BP at times exceeding 200 mm Hg systolic and >110 mm Hg diastolic) — qualifies her as a true hypertensive emergency (Janke et al — JAHA 5(12); 2016 — and — Cardiology Advisor — Feb. 29, 2024). Fortunately — today's patient rapidly responded to initiation of IV NTG.
- It is not always appreciated that chest pain is one of the most common associated symptoms of hypertensive crisis presenting to the ED (occurring in more than half of the patients with HT urgency — and in an even greater percentage of those with HT emergency in the study by Salkic et al — Mater Sociomed 26(1):12-16, 2014).
- PEARL: Case #1 in today’s post provides superb illustration of the synergistic effect that IV NTG may have in the patient who presents with severe CP in association with the combination of hypertensive emergency and acute MI.
-USE.png) |
| Figure-1: I've labeled the initial ECG in Case #1. |
- We have often made the point in Dr. Smith's ECG Blog that in general — it is not common to see tachycardia with an uncomplicated MI. As a result — the finding of sinus tachycardia in today's case should immediately suggest that something else might also be going on (which in today's case was this patient's severe CP and her hypertensive emergency).
- This degree of increased S wave amplitude made me initially stop to consider proportionality of the amount of chest lead ST elevation relative to the increase in chest lead voltage.
- Double RED arrows in leads V3,V4,V5 highlight what I considered the point of inflection defining the J-point for determining the amount of ST elevation. Even in lead V3 (in which the S wave attains a depth of 36 mm) — the 8 mm of J-point ST elevation is inappropriately increased, and indicative of acute MI in this patient with severe new CP.
- S wave depth is much less in neighboring leads V4 and V5 — which clearly show disproportionate J-point ST elevation (of 12 mm and 9 mm in lead V4 and lead V5, respectively) — compared to more modest S wave depth in these leads (ie, of 20 mm and 11 mm). As per Dr. Smith — the overall ECG picture in Figure-1 indicates an anterior STEMI in progress in this patient with acute hypertensive emergency.
- While difficult to know what to make of inferior lead ST-T wave appearance — the inappropriate T wave inversion in lead aVL adds further support to the diagnosis of an ongoing STEMI.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.