
Written by Willy Frick
A middle aged man presented for elective outpatient surgery. The following ECG was obtained in the preoperative area.

What do you think?
The ECG shows sinus rhythm with a rate of about 78 and 2:1 AV conduction along with right bundle branch block and left anterior fascicular block. The PR interval on the conducted beats is prolonged, about 220 ms. Eagle eyed readers might notice PP interval variation.
One differential diagnosis would be blocked PACs, a common cause of pauses on ECGs. However, given that the P waves are all identical in morphology, the more likely explanation is the ventriculophasic response. The exact mechanism is subject to debate, but the characteristic finding is that PP intervals which contain a QRS complex are shorter than PP intervals which lack one. That is exactly what we see here. It can be seen in other forms of heart block as well (such as complete heart block). See Ken Grauer's comment below for more on this.
As this patient is scheduled for imminent elective surgery, it is important to determine whether this is Mobitz I (benign) or Mobitz II (requires pacing).
So...Which is it?
Answer: You cannot be certain from this ECG alone.
The usual way to discriminate between Mobitz I AV block and Mobitz II AV block is by comparing successive PR intervals. If there is PR prolongation from one to the next, this supports Mobitz I physiology which rarely benefits from pacing. Conversely, if the PR interval is constant, this supports Mobitz II physiology, which is an indication for pacing. 2:1 block is a special case, because the tracing lacks successive PR intervals. This pattern can be seen in both Mobitz I and Mobitz II physiology.
History is often helpful. If the patient is otherwise healthy and has a good reason to have high vagal tone (like nausea or somnolence), it is likely Mobitz I. On the other hand, history of syncope does not necessarily prove that it is Mobitz II. This is because high vagal tone can cause reflex syncope, as in this case.
You can also use bedside maneuvers to investigate further. Interventions which increase vagal tone tend to worsen Mobitz I block. Perhaps surprisingly, vagal maneuvers can actually improve conduction in Mobitz II block. This is because the slower sinus rate gives more time for the His-Purkinje system to recover. The opposite is true for maneuvers which reduce vagal tone (i.e., they improve conduction in Mobitz I and worsen it in Mobitz II).
So, for example: atropine and exercise should both improve conduction in Mobitz I block, but make it worse in Mobitz II. Conversely, carotid massage should worsen conduction in Mobitz I block, but make it better in Mobitz II.
In this case, you might suspect Mobitz II block since there is already infra-Hisian disease manifest with the bifascicular block. But this is only a guess. As it turns out, the patient had a repeat ECG obtained prior to evaluation by cardiology.

What do you think?
This is an extremely helpful ECG, because we now have two successive PR intervals to compare to each other (P-waves preceding QRS complexes 4 and 5). I have labeled the P waves below for ease of reference:
P waves 8 and 9 both conduct to the ventricles. You can probably tell just by eyeballing, but caliper measurement confirms that there is PR prolongation, thus confirming Mobitz I block.
So, should the patient go to surgery?
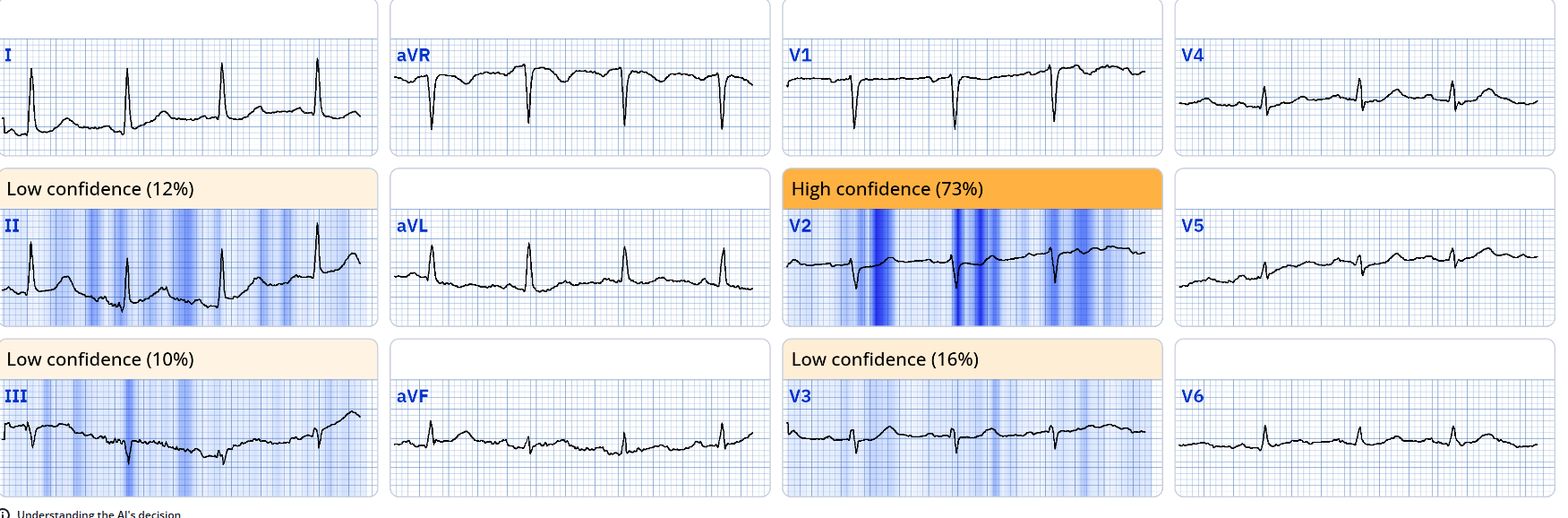
In order to test the hypothesis further, cardiology performed carotid massage while recording 12 leads of rhythm. This is shown below:

A few seconds into the strip you can see the carotid massage artifact (most pronounced in V1-2). Quite surprisingly, carotid massage slows the sinus rate slightly, and as a result instantly improves AV conduction to 1:1, supporting Mobitz II AV block!
The patient went for EP study and had prolonged HV interval which strongly supports placement of a pacemaker. He underwent dual chamber pacemaker implantation and did well.
Learning points:
- Mobitz I and Mobitz II can co-exist in the same patient at the same time
- Bedside maneuvers can help clarify the etiology of 2:1 AV block
===================================
MY Comment, by KEN GRAUER, MD (11/12/2024):
===================================
Questions often arise regarding the various forms of 2nd-degree AV block. Today's case proves insightful, not only by reviewing KEY concepts on this subject — but also by illustrating a case in which bedside maneuvers can help to distinguish between the types of 2nd-degree AV block — and, in which the patient "did not read the textbook".
- I focus my comment on some additional advanced concepts to those discussed in Dr. Frick's excellent review.
- As per Dr. Frick — some history is needed, especially since some patients are at times less than forthcoming with a history of presyncope or syncope unless probing questions are asked.
- Finding a previous ECG from this patient for comparison would be tremendously helpful (Are the conduction defects new or old?).
- To Emphasize: This elective pre-op ECG is not normal. Even if the 2nd-degree AV block is not initially recognized — there are several significant ECG abnormalities (as highlighted by Dr. Frick) which include 1st-degree AV block (PR interval = 0.24 second) — and bifascicular block in the form of RBBB/LAHB.
- More subtle, but equally important — is the question of when these ECG abnormalities may have occurred? The small-but-definitely-present initial q wave in lead V2 (within the dotted RED circle in Figure-1) is not a normal finding with this RBBB considering that there definitely is a typical triphasic (rsR' ) QRS complex in neighboring lead V1 (ie, So there has been loss of the initial r wave that was seen in lead V1 ).
- Further support that anterior infarction of unknown age may be the cause of the above noted conduction system abnormalities — is forthcoming from the ST segment flattening in multiple leads (BLUE arrows) that is not a typical finding with bifascicular block unless there is underlying heart disease. And although the inferior lead T wave inversion could simply be the result of the predominantly negative QRS complexes of the LAHB — ruling out recent MI seems advisable prior to approval for elective surgery.
- Finally — Regardless of whether the 2:1 AV block is seen — there is marked bradycardia (rate in the 40s), which of itself deserves investigation prior to approval for elective surgery.
- Therefore: The "quick" answer to today's case (obvious within seconds) — is that further evaluation (and potential pacemaker placement) is needed prior to approval for elective surgery.
==============================
What follows is a "deep dive" into some of the intricacies of the 2nd-degree AV block for readers with an interest in advanced arrhythmia interpretation.
==============================
Did YOU See the 2:1 AV Block?
Over the years — I've occasionally encountered tracings for which an unexpected 2:1 AV block makes me STOP for a moment to verify that the rhythm in front of me truly is 2:1 block (and not some masquerading T wave or U wave). This was the case for today's rhythm — for which the marked bradycardia made me suspect 2:1 conduction — but for which the deceptively flat T waves in multiple leads (See the BLUE arrows in leads V4,V5,V6 of Figure-1) made me initially question what was T wave vs U wave vs "extra" P wave vs some superposition of both? And, before cancelling a scheduled elective surgery (with the patient already prepped in the pre-op room) — I would want to be 100% certain that I was truly looking at 2:1 AV block.
- The timing of the potenial "extra deflection" is critical. Using calipers is the fastest and easiest way to check IF what appears to be an extra P wave deflection is real (and not just a look-alike T wave or prominent U wave).
- As can be seen from the RED arrows in Figure-1 — the timing of these potential P wave deflections is consistent with the presence of an extra P wave.
- One needs to be aware of the phenomenon known as ventriculophasic sinus arrhythmia. It is common with both 2nd- and 3rd-degree AV block to see some variation in the P-P interval beyond that expected with a simple sinus arrhythmia. The proposed rationale for this "ventriculophasic" P-P interval variation — is that the P-P interval that contains a QRS complex "sandwiched" within it, tends to be slightly shorter than the P-P interval located away from the QRS — because coronary perfusion will be a little better immediately following ventricular contraction.
- As per the P-P intervals (in milliseconds) that I have meticulously measured in the lead V5 rhythm strip in Figure-1 — a subtle ventriculophasic sinus arrhythmia is seen in today's case (and it "fits" the typical model of slightly shorter P-P intervals when a QRS is contained within).
- PEARL: The real benefit of being aware of ventriculophasic sinus arrhythmia — is that because the variable P-P interval gently offsets the location of the non-conducted P wave — this allows greater certainty that the potential extra deflection is truly a P wave (ie, This is BEST appreciated in the long lead V1 rhythm strip in Figure-1). Whereas it might be difficult at first glance to distinguish the extra P wave from the T wave in leads II and V5 — Isn't it much easier to recognize the distinct biphasic P wave shape for each P wave in the long lead V1? A T wave would not produce this rounded, terminal negative deflection that so perfectly matches the terminal rounded negative deflection of the sinus P waves before each QRS — such that on seeing this picture in lead V1 — I knew that the rhythm was 2nd-degree AV block with 2 P waves for each QRS complex.
.png) |
| Figure-1: I've labeled the initial ECG in today's case. (To improve visualization — I've digitized the original ECG using PMcardio). |
The 3 Types of 2nd-Degree AV Block:
Many textbooks still break down the 2nd-degree AV blocks into 2 categories: Mobitz I vs Mobitz II. Instead, I have always favored Marriott's approach for description of the 2nd-degree AV blocks. According to Marriott — there are 3 (not 2) Types of 2nd-degree AV block. These are:
- Mobitz I (which is the same thing as AV Wenckebach) — in which there is progressive PR interval prolongation until a beat is dropped.
- Mobitz II — in which the PR interval is constant, until one or more beats are dropped.
- 2:1 AV Block — in which it is impossible to be certain whether the type of 2nd-degree AV block is Mobitz I vs Mobitz II. As per Dr. Frick — the clinical importance of this distinction — is that Mobitz I is much more likely to be benign (dependent of course on clinical circumstances) — whereas Mobitz II is much more likely to need pacing (because of the disturbing tendency of Mobitz II to suddenly drop conduction of not one, but multiple successive complexes — potentially resulting in ventricular standstill).
How to Tell Mobitz I vs II when there is 2:1 AV Block?
The above said — most of the time we can with high accuracy distinguish between Mobitz I vs Mobitz II — simply by keeping the following clinical features in mind:
- Mobitz I is much more common than Mobitz II. While relative percentages of these 2 conduction disturbances may vary, depending on whether your practice is EP cardiology — outpatient medicine — or treating patients who present for acute care — Statistics strongly favor Mobitz I (ie, Over the 4+ decades that I've studied all AV blocks that have come my way — well over 90% turn out to be Mobitz I ). It's essential not to overlook the Mobitz II cases (because referral for pacing is needed) — but statistically, the overwhelming majority of cases non-EP-cardiologists will see will turn out to be Mobitz I.
- The reason Mobitz I has a much better overall prognosis — is that this rhythm disturbance occurs at a higher level within the conduction system (usually within the AV Node). As a result — Mobitz I usually manifests a narrow QRS (unless there is underlying BBB) — Mobitz I is more likely to be influenced by increased vagal tone, and it tends to respond well to Atropine when given during the early hours of acute inferior MI (during which vagal tone is often temporarily increased) — with acute inferior MI probably being the most common clinical situation in which Mobitz I is seen. That said — there are occasions when even Mobitz I 2nd-degree AV block needs permanent pacing (ie, when Mobitz I is associated with marked bradycardia and/or the patient is clearly symptomatic).
- In contrast — Mobitz II occurs lower down in the conduction system. As a result — Mobitz II is most often seen with acute anterior MI — there typically is QRS widening (with either BBB and/or hemiblock) — and atropine is unlikely to be effective.
- In general — the PR interval is more likely to be normal with Mobitz II.
- In contrast — the PR interval is more likely to be prolonged with Mobitz I. This is because with those cases of acute inferior MI that develop AV block — there is often a sequential development of conduction disturbances. That is, there tends to be sequential progression from a normal PR interval — to 1st-degree AV block — to Mobitz I — and on occasion, to 3rd-degree block at the AV nodal level (ie, with a narrow QRS). And, when the AV conduction disturbance with these inferior MI patients resolves — it tends to do so in reverse progression (ie, regressing from 3rd-degree — to Mobitz I 2nd-degree — to 1st degree — until there finally is restoration of sinus rhythm with a normal PR interval).
- In general — it is uncommon (rare in my experience) — for a patient to go back-and-forth between Mobitz I and Mobitz II forms of 2nd-degree AV block. Therefore — if you see clear evidence of Mobitz I elsewhere on telemetry monitoring (ie, the 3:2 Mobitz I sequence highlighted by Dr. Frick on today's 2nd tracing) — this usually very strongly suggests that those periods of 2:1 AV block are also a manifestation of Mobitz I.
- KEY Point: Dr. Frick skillfully illustrates in today's case how this usually helpful indicator that the block is Mobitz I fails to hold true in today's case — because both Mobitz I and Mobitz II co-exist in today's patient (who I like to say — "failed to read the textbook" before coming to the hospital).
- Also in today's case — Statistics are wrong — because despite how much more common Mobitz I is than Mobitz II (and despite the prolonged PR interval that is so commonly seen with Mobitz I ) — today's patient also had Mobitz II.
- Then again — the bifascicular block (RBBB/LAHB) and suggestion of anterior MI at some point in time (the abnormal Q wave in V2 in association with multiple conduction disturbances and abnormal ST-T flattening in multiple leads) are factors in favor of Mobitz II.
- Finally — the ingenious use of bedside maneuvers (as described by Dr. Frick) provides a way to suspect in today's case that this patient may turn out to be one of the rare patients in whom Mobitz I and Mobitz II co-exist!
CASE Conclusion: While the need to defer elective surgery and refer today's patient for further evaluation should be obvious within seconds of seeing today's initial ECG — Close scrutiny of the details of today's case makes for a fascinating adventure in advanced arrhythmia interpretation with important lessons for clinical application. Our THANKS to Dr. Frick for sharing this case!






-USE.png)
-USE.png)




-USE.png)
-USE.png)
-USE.png)
-USE.png)
-labeled-USE.png)
-USE%20.png)
-LADDERGRAM-USE.png)
-USE.png)
-labeled-USE.png)
{kind=link}
{kind=link}