
Written by Magnus Nossen, with some edits by Smith
This ECG was transmitted electronically by EMS for evaluation. The patient is a 70 something female with chest discomfort and dyspnea. How would you interpret the ST changes seen in this ECG? Will you accept this patient for emergent coronary angiogram based on the ECG changes? Does the ECG represent STEMI-negative OMI findings? How would you mange this patient?

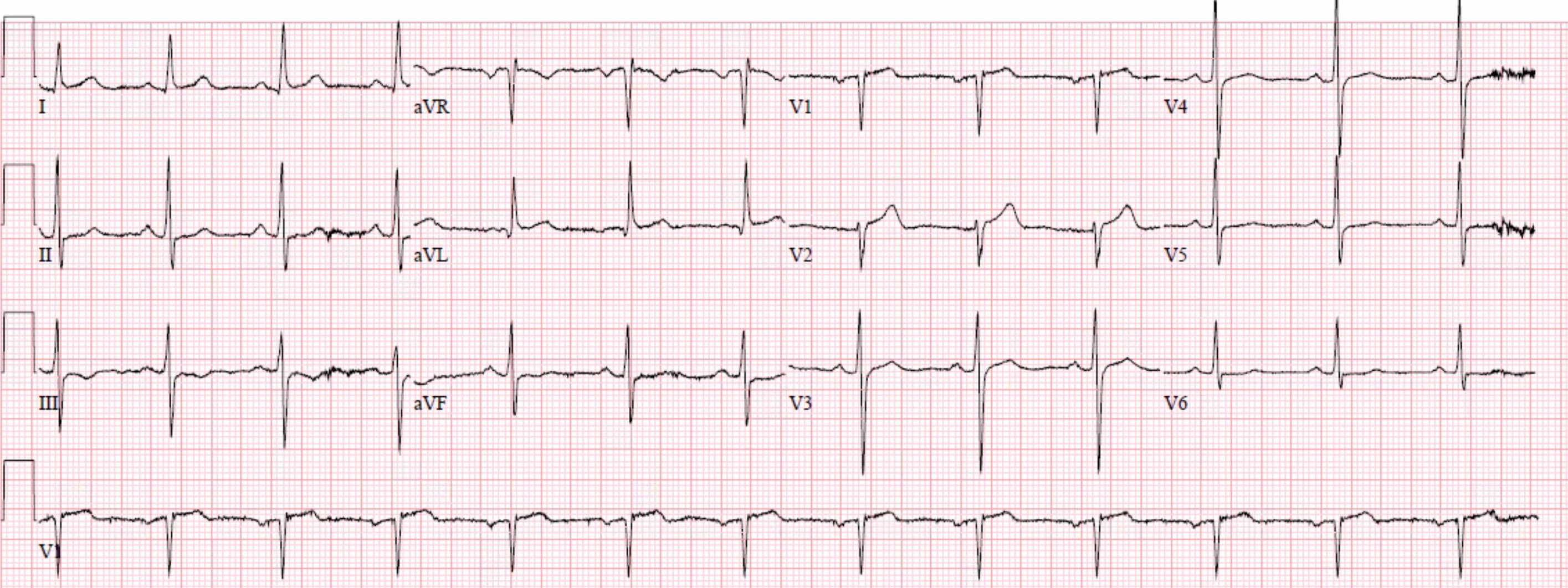
The ECG shows sinus rhythm with a ventricular rate just below 100 bpm. There is slight concave ST segment depression in the inferior leads with trace ST elevation in lead aVL not meeting millimeter criteria. Of note also is delayed R-wave progression in the anterior leads without significant Q-waves. P-waves are prominent. It would be reasonable to evaluate this patient in a PCI center as you have to prove that these ECG changes are not ischemic. I accepted the patient for evaluation in our PCI facility but did not activate the cath lab as I did not think the ECG changes represented OMI.
Smith: The P-wave in lead II is extremely prominent, suggesting right atrial hypertrophy and possible high right sided pressures.
ST depression has a variety of different causes. The cause can be primary, (i.e ischemia) or it can be secondary to abnormal depolarization (e.g from preexcitation, BBB, paced rhythm, LVH etc).
Furthermore, ST depression can be caused by drugs (e.g digoxin) or electrolyte imbalances such as hypokalemia or hypomagnesemia. Even certain rare hereditary arrhythmogenic disorders like Bundgaard syndrome can have ST depression in the resting ECG.
Discussion: The ECG in today's case does not have typical ST depression vector of diffuse subendocardial ischemia. The ST vector in subendocardial ischemia (SEI) usually has the largest amount of ST depression in leads II and V5, towards the apex of the heart. (ST depression vector towards II and V5). In fact, the ST depressions in the ECG in today’s case are most pronounced in the leads with the largest P waves (!) and not in the leads with the largest amplitude QRS complexes. This is a very strong indicator that the ST-depression is not ischemic but rather related to the P wave size and vector.
The patient was evaluated immediately upon arrival. Physical exam was notable for wheezing bilaterally. She had known severe COPD. Bedside echo was without wall motion abnormality.
Putting all the findings together; dyspnea, slight tachycardia, delayed R-wave progression, prominent lateral S waves and ST depression maximal where the P waves are largest all point toward pulmonary disease as the cause of the ECG findings.
Atrial repolarization is usually not noticed on the ECG. However, if atrial enlargement occurs, atrial repolarization may become prominent and may cause ST segment changes. Figure A below shows the relationship of the Ta wave to normal ST depression. In figure B below I have superimposed a red dotted parabolic line on the QRS complexes and ST segments of leads aVL and aVF to show how the atrial repolarization wave affects the ST segments.
Figure A


How did the QoH perform on this ECG?


It is quite impressive how the interpretation is NOT OMI with high confidence. Above you can see the explainability feature. The AI model does not react to any of the ST segments in this ECG.
You too can have the Queen of Hearts AI model
Learning points:
- The ECG often can give clues to pulmonary disease
- Atrial repolarization wave (Ta wave) can mimic ischemia.
- ST depression has a variety of different causes other than ischemia.
MY Comment, by KEN GRAUER, MD (5/31/2024):
- I count among my favorite sayings the following: "Experience is Errors". Much of what I have learned over the decades that I've been studying ECG interpretation, is the result of "errors" committed that I have learned from. And so, I'll never forget as an intern how I assumed after numerous pulmonary edema cases — that the dyspneic patient in front of me was yet one more patient in need of diuresis and other standard left-sided heart failure measures. I misdiagnosed that patient's ECG — which was "trying" to tell me that rather than left-sided heart failure — the problem was right-sided failure from longstanding severe pulmonary disease. I have tried not to make that mistake again.
- We do not often see RVH on ECG in adults. As a result — it is easy to overlook this important clue to right-sided heart failure. This essential clinical message is superbly conveyed by today's case.
-USE%20copy.png) |
| Figure-1: I’ve labeled findings potentially consistent with RVH — from the initial ECG in today case. |
- Among the most challenging of ECG diagnoses to make is RVH (Right Ventricular Hypertrophy). By saying this — I am not referring to obvious cases of ECG RVH — in which the QRS is of normal duration (ie, No RBBB and no WPW) — and there is marked RAD (Right Axis Deviation) + a predominant R wave in lead V1.
- KEY Point: The extreme ECG findings of marked RAD and predominant R wave in lead V1 are usually not found in adults with RVH until late in the course — and sometimes not even then. Instead — I am referring to less obvious, but still clinically significant forms of RVH that are all-too-easy to overlook!
- RVH is much easier to diagnose in infants and young children than in adults. This is because the relative size (and mass) of the RV (Right Ventricle) compared to the LV (Left Ventricle) — is much greater in infants and young children compared to adults. In contrast, by the time adulthood is reached — the normal LV may be up to 3X as thick (with up to 10X the mass) of the normal RV. As a result — a marked increase in RV size is usually needed in adults — before a predominant R wave will be seen in lead V1.
- In contrast — an R>S ratio (ie, R wave height greater than S wave depth) in lead V1 — remains a common and normal finding in children up until ~5 years of age!
- Similarly (ie, because of the normal LV predominance) — marked RAD in the frontal plane is a relatively late sign of RVH in adults.
- I’ve reviewed My Take on the ECG diagnosis of RVH on a number of occasions in Dr. Smith’s ECG Blog (See My Comment at the bottom of the page in the March 6, 2022 and September 1, 2020 posts, to name just 2).
- As review — my user-friendly summary of ECG RVH appears in the ADDENDUM below (in Figures-2-thru-5).
- PEARL #3: As is often the case — the History is KEY! Today's patient presented not only with chest pain — but also with dyspnea. Later in the case we learned that she indeed had longstanding severe pulmonary disease — therefore consistent with a patient having potential RVH.
- Marked RAA (Right Atrial Abnormality) is present! The tall, peaked and pointed P waves in each of the inferior leads (that easily surpass the ≥2.5 mm tall voltage criteria) — clearly establishes the presence of RAA, which in a patient presenting with acute dyspnea indicates right atrial enlargement.
- PEARL #4: There is only 1 condition in medicine that produces right atrial enlargement without also producing RVH. That condition is tricuspid stenosis, which is rare. Therefore, the ECG finding of RAA that is not the result of slender body habitus — provides an important presumptive clue to the presence of RVH.
- The Axis: While frank RAD is not present — the normal QRS complex in lead I is positive. Low amplitude of the R wave that we see in lead I of Figure-1 — in association with an S wave of equal (if not greater surface area) compared to the R wave in this lead is not a usual finding.
- S Waves in Leads I, II, and III: This finding is related to the mean QRS axis in today's tracing. Seeing S waves in each of the standard limb leads (as we see in Figure-1) of itself suggests significant pulmonary disease — as does the resultant, almost indeterminate QRS axis.
- Relatively Low Voltage: While strict criteria for low voltage are not present (ie, All 6 limb leads ≤5 mm) — overall QRS amplitude looks reduced in the limb leads of Figure-1.
- Persistent S Waves: R wave amplitude normally increases as one moves across the precordial leads (as electrical activity moves toward the left where the larger LV lies). R wave amplitude usually peaks in V4 or V5 — and then drops off (in V5,V6). Normally, there is not any S wave at all in V5,V6 — since by this time in the depolarization process, all electrical activity is traveling leftward. If more than tiny S waves are still present in V5,V6 — this may be the result of significant ongoing rightward activity.
- Lead aVR: Acute RV overload may be reflected on ECG by ST elevation in lead aVR (especially when the R wave in lead aVR is tall, as it is in Figure-1).
- While fully acknowledging that the QRST complex in lead I of Figure-1 does not satisfy the very low millimeter size criterion for Schamroth's Sign — Isn't this QRST complex in lead I quite small? I seized upon this subtle finding as yet another clue to the likely diagnosis of severe pulmonary disease rather than OMI in today's case.
===============================
- “My Take” on the ECG diagnosis of RVH appears in the following 4 Figures (from Grauer K: ECG-2014 e-Pub).
 |
| Figure-2: ECG Criteria for RVH. |
 |
| Figure-3: ECG Criteria for RVH (Continued). |
 |
| Figure-4: ECG diagnosis of pulmonary disease and RVH in children. |
 |
| Figure-5: Example tracings of RVH. |










-USE%20copy.png)











-USE.png)