
This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech. The undergraduate is now willing to identify himself: Hans Helseth.
On the second morning of his admission, he developed 10/10 chest pain and some diaphoresis after breakfast.
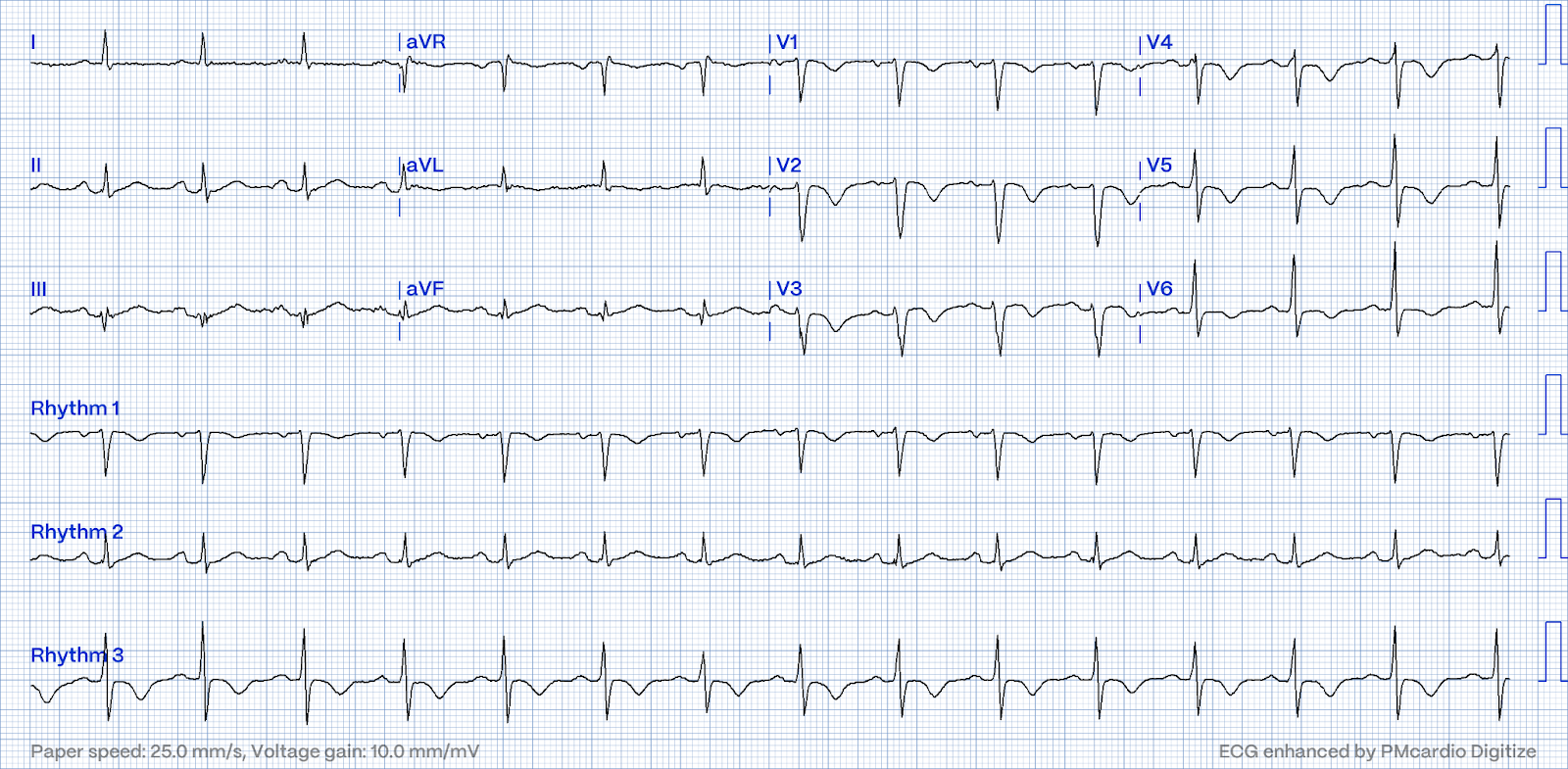
An EKG was taken at 0917:

The conventional computer algorithm (Marquette 12 SL) diagnosed “Normal Sinus Rhythm, Normal ECG”:
What do you think?

This is clearly very different, and confirms that the above ECG has hyperacute T-waves.
See the side-by-side comparison at the bottom
The consulting cardiologist noted no change between this EKG and the latest, confirming the computer's “normal” read and calling the latest EKG “unremarkable” in the consult note. The anterior T waves are now, however, noticeably bulkier than in the old ECG.
The Queen of Hearts does not see the hyperacute T waves. She reads Not OMI with high confidence:
Smith: I am very surprised that she did not see these hyperacute T-waves. She is usually incredibly good at recognizing them! On some occasions, expert humans are better than the Queen of Hearts!
The patient was given opiates which improved his chest pain to 7/10. At 1010, the first troponin I (URL 0.034 ng/mL) returned elevated at 0.4 ng/mL.
At 1321, a repeat troponin I returned at 0.62 ng/mL. Another EKG was taken at 1454:

It is unclear whether or not the patient had pain at this point, but the EKG suggests reperfusion of the anterior wall. The T waves have deflated significantly and V2 shows the terminal T wave inversion typical to reperfusion.
Smith: These are pathognomonic in this clinical situation, and identical to Wellens' Pattern A biphasic T-waves
The conventional computer algorithm diagnosed “nonspecific T wave abnormality.” The cardiologist noted “T waves appear flatter in precordial leads.”
The Queen of Hearts again diagnosed Not OMI with high confidence.
Smith: Again, I am very surprised by the Queen. I suspect that Version 2 would do better and that will be released soon.
The consulting cardiologist wrote in their note:
“Could be cardiac chest pain. EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain”
At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum.
A plan was made to put the patient on heparin and continue to trend troponins. At 1605, another repeat troponin resulted at 5.271 ng/mL. The patient received a diagnosis of “NSTEMI” and angiography was scheduled for the next day.
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). An EKG was repeated around midnight:

But in the context of the previous EKGs, it suggests re-occlusion of the LAD culprit. This is pseudonormalization. The patient’s pain status at this point is also unclear, but one might expect that his pain has returned based on contextual evidence of re-occlusion.
The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia.
The conventional computer algorithm called “sinus tachycardia, otherwise normal EKG”. The cardiology overread wrote in comparison to the EKG taken at 1454, “QT has lengthened, nonspecific T wave abnormality is resolved”.
Smith: The Queen of Hearts diagnosed Not OMI with high confidence. The computer algorithms do not have the advantage of "seeing" the previous ECG. Not yet anyway.
At 1742 the next day, a final EKG was taken before angiography:

This EKG again shows reperfusion of the anterior wall. Notably, the precordial R wave progression has worsened, suggesting infarction of the anterior wall.
These are Wellens' Pattern B waves (deep symmetric). Pattern A evolves into Pattern B.
See this post: Classic Evolution of Wellens' T-waves over 26 hours
The Queen of Hearts recognized reperfusion here, diagnosing OMI with low confidence.
Smith: Version 1 diagnoses OMI even if it is reperfused OMI. Version 2 will not do this.
Finally, at 1823 on the patient’s third day of admission (33 hours after the first diagnostic EKG) the patient was taken for angiography:
RAO Cranial view

The red arrow points to a 90% stenosis in the proximal segment of the LAD. The lesion had TIMI III flow on angiography, consistent with the spontaneous reperfusion seen on the last EKG before cath.
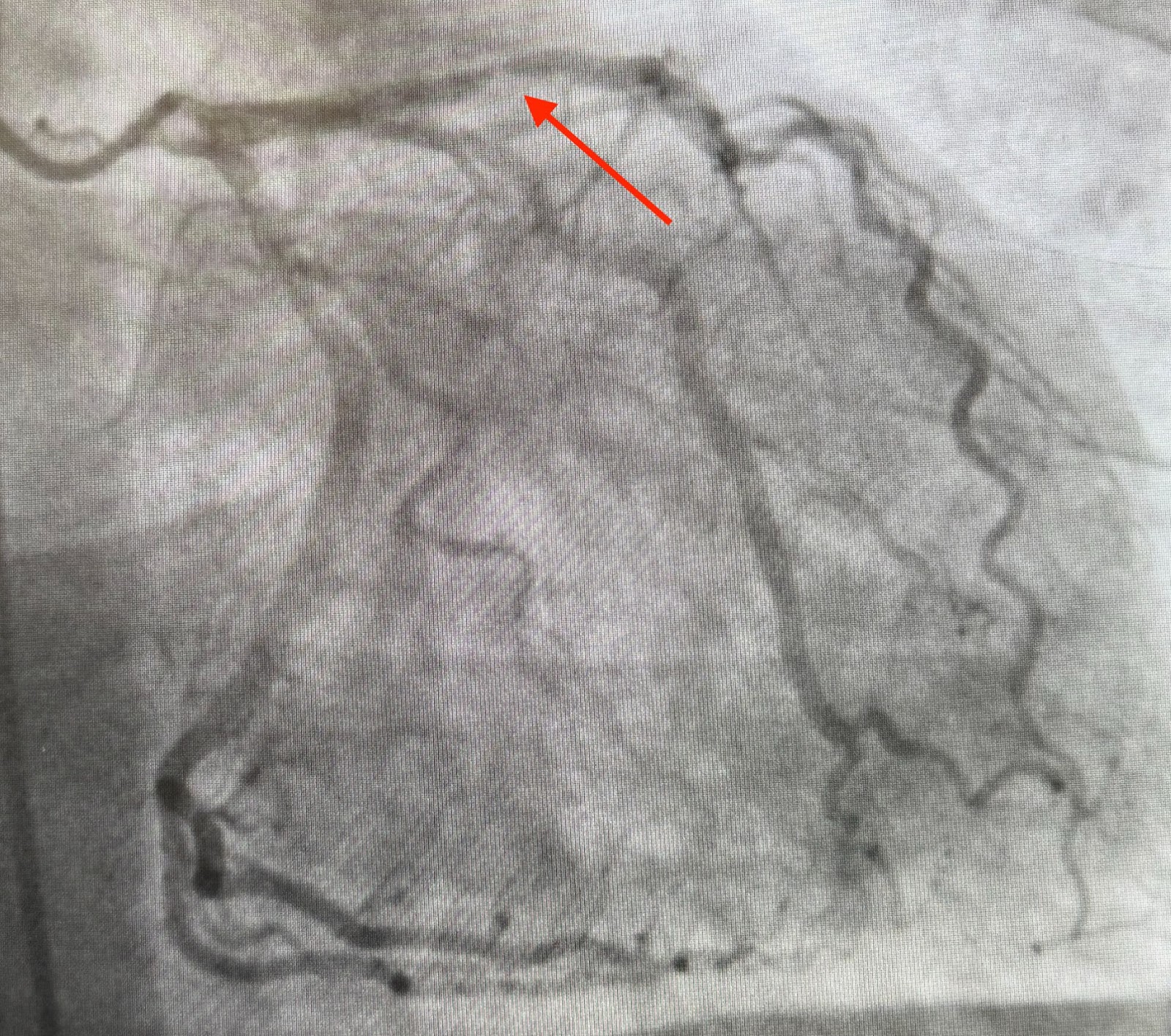
This is the RAO Caudal view. The red arrow indicates the culprit lesion in the proximal LAD.

This is the RAO Caudal view after thrombectomy and stent placement. The proximal LAD is now widely patent.
The rest of the patient’s hospital stay was uneventful and he was eventually discharged. This photo shows the series of occlusion and reperfusion the patient underwent during his hospital stay as seen in the right precordial leads:
 |
| Not only are T wave changes apparent, but the R waves can be seen to decrease in size. |
MY Comment, by KEN GRAUER, MD (9/25/2024):
- Regular readers of this ECG Blog will be well familiar with many of these points. Nevertheless, cases like the one presented today — illustrate the continued need for review of these points that are KEY to attaining a good outcome.
- For clarity in Figure-1 — I've put together today's initial ECG — with this patient's baseline ECG done a year earlier.
- This 56-year old man with risk factors including diabetes and known coronary disease — presented to the ED on Day #1 with new weakness, fatigue, lethargy and confusion.
- No ECG was ordered on Day #1.
- On the morning of Day #2 — the patient suddenly developed 10/10 CP (Chest Pain) shortly after breakfast. This prompted the ordering of the patient's 1st ECG ( = ECG #1 done at 9:17am — as shown in Figure-1).
- Cardiology was consulted — and interpreted ECG #1 as "unremarkable". Cardiology agreed with the computer interpretation that said, "Sinus rhythm; Normal ECG".
- Cardiology gained access to the patient's baseline tracing ( = ECG #2) — and said there was "no change" in today's initial tracing compared to the baseline ECG done a year earlier.
- The patient was treated with opiates for his 10/10 CP. Use of opiates resulted in reduction of the patient's CP to a severity score of 7/10.
- At 10:10 am ( = 53 minutes after ECG #1 was done) — the 1st Troponin came back elevated = 0.4 ng/mL (upper normal = 0.034 ng/mL).
- The 2nd ECG on this patient was not obtained until 14:54 ( = 4+ hours after the elevated 1st Troponin value — and 5+ hours after the 1st ECG).
- How many of these errors can YOU identify?
 |
| Figure-1: Comparison between today’s initial ECG — with the baseline ECG from ~1 year earlier. |
- An ECG should be routinely ordered at the time the patient is admitted to the hospital whenever the patient presents with new symptoms (such as the weakness — fatigue — lethargy — and confusion that were noted in today’s case). More than simply “ordering” an admission ECG — the treating clinician should look at this admission ECG when examining the patient. Doing so in today’s case might have expedited recognizing the need for cardiac cath by more than a day!
- As I periodically highlight in Dr. Smith's ECG Blog — the entity of “silent” MI is much more common than is often appreciated (See My Comment in the August 19, 2023 post, among many others). Framingham taught us that ~1/2 of all “silent” (ie, non-CP) MIs have “something else” (ie, some other non-CP symptom). This is relevant to today's case — because a history of new weakness — fatigue — lethargy — and/or confusion — have each been known on occasion to be the presenting symptom of a “silent” MI.
- Given that today's patient has known coronary disease — sudden development of 10/10 CP immediately places this patient in a much higher-prevalence group for having an acute coronary event. As a result — regardless of whether the initial ECG and initial Troponin values come back normal — additional evaluation will be needed to rule out an acute event. This was not done (ie, The 2nd ECG was not obtained in today's case until 5+ hours after the 1st ECG — whereas the 2nd ECG should have been obtained within 10-30 minutes after ECG #1).
- In a patient with new-onset 10/10 CP — the initial ECG in today's case can not be interpreted as "normal" or "unremarkable" (as it was by Cardiology). Instead — a subtle but-clearly-seen straightened ST segment takeoff is present in all 3 anterior leads (within the RED rectangle — being most marked in leads V2, and V3, but also seen in lead V1). Especially in leads V2 and V3 — the T wave is "fatter"-at-its-peak and wider-at-its-base than should be expected given relative QRS amplitude in these leads. As per Dr. Smith — these findings are diagnostic of acute LAD OMI. The cath lab should have been immediately activated at this point!
- As I have often emphasized in this ECG Blog — unless serial ECGs are placed side-by-side when they are compared — important findings will be missed. In Figure-1 — Isn't the shape of the ST segment takeoff and the relative volume of the ST-T waves in leads V1,V2,V3 clearly different when comparing the 3 leads within the RED and BLUE rectangles? This is because in a patient with new CP — the ST-T waves in leads V1,V2,V3 of ECG #1 are hyperacute (ie, indicative of acute LAD OMI until proven otherwise).
- In any case — the ECG in today's case should have been repeated within 10-30 minutes.
- Opiates should not be used to treat CP until: i) The decision has been made to immediately activate the cath lab; — or, ii) A definitive diagnosis of a non-cardiac cause of CP has been made that merits treatment with narcotics (ie, if CP turned out to be the result of cancer). The reason is that if opiates relieve the CP of acute coronary occlusion — then the needed cardiac catheterization for PCI might not get done if the patient's CP was gone. (For more on use of Opiates with acute ischemic CP — See the January 6, 2023 post in Dr. Smith's ECG Blog).
- That said, in today's case — CP was only modestly reduced by opiates (ie, from 10/10 to 7/10). Even if the initial ECG would have been normal (which it wasn't) — persistence of 7/10 CP that is thought to be ischemic — by itself would be indication for prompt cath.
- The fact that the 1st Troponin came back elevated further supports the previous bullet — which states, that even if the initial ECG would have been normal — persistence of ischemic CP in the face of an elevated Troponin is indication for prompt cath.
- IF for any reason the initial ECG (that was done at 9:17am) had not yet been repeated — return of an elevated Troponin (at 10:10am) should have immediately prompted repeat ECG.
- There are many lessons to be learned from today's case.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.