
Case submitted and written by James Tavornwattana, edits by Pendell Meyers and Steve Smith
A male in his 60s with diabetes presented to the ED with one hour of palpitations associated with a 30 min episode of throat burning sensation when he woke up this morning. He denied chest pain, shortness of breath, or lightheadedness.
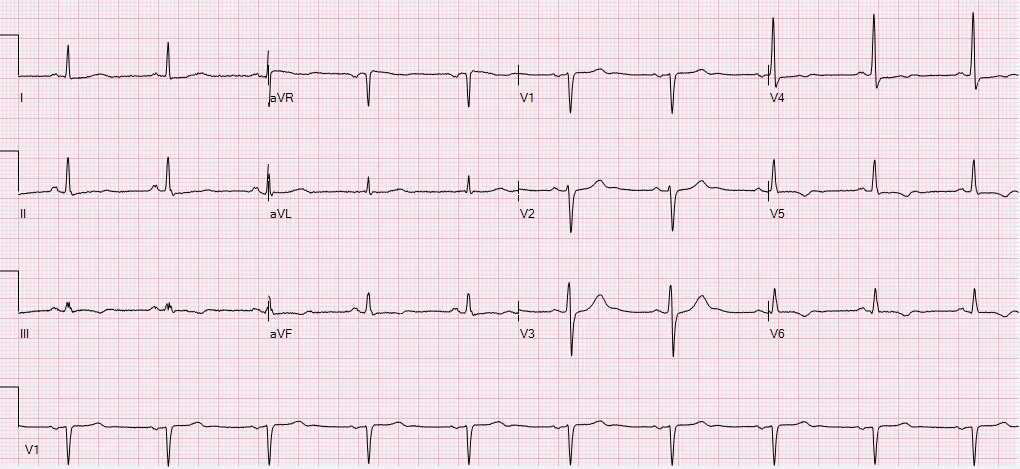
Interpretation:
Atrial fibrillation with rapid ventricular response
Back to the case:
The clinicians thought the STD represented demand ischemia from AF with RVR. The patient was given magnesium, diltiazem, and fluids with improvement in ventricular rate. Unfortunately there is no ECG recorded soon after rate control. This would be important to see if the posterior ischemia has resolved with rate control or not.

Troponins continued to rise with peak 0.67 ng/mL at about 24 hours from presentation. Echo showed moderated to severe mid to basal inferolateral wall hypokinesis (What is commonly referred to as the posterior wall). Apparently at this time the patient was no longer symptomatic, so cath was scheduled for the next morning.
The cath showed a complete thrombotic occlusion of the LCX (collateral flow was not commented on, but could have been present). The LCX was stented open with good angiographic result. There was also other chronic CAD in various vessels without any other acute culprits.
Here is the post-cath ECG:

Roughly the same as before the cath.
The patient did well.
Learning Points:
When there are multiple leads with STD, then you must find where the STD is maximal. STD maximal in V1-V4 is posterior OMI until proven otherwise. Diffuse supply/demand mismatch ischemia presents with STD maximal in V4-V6 and lead II (the average overall axis of depolarization), and therefore must always also present with STE in aVR.
See this diagram that highlights this learning point:

When ECG findings of OMI are present in the setting of AF with RVR, one of the initial steps in management is to control the rate which will reduce supply demand mismatch and allow for a repeat ECG at reduced heart rate (with better quality and the chance to see if the ischemic findings have resolved with reduced rate).
See this similar case:
A male in his 60s with diabetes presented to the ED with one hour of palpitations associated with a 30 min episode of throat burning sensation when he woke up this morning. He denied chest pain, shortness of breath, or lightheadedness.
Initial ECG (0 hr):
 |
| What do you think? |
Interpretation:
ST depression that is maximal in V2-V4, also with lesser STD in V5, I, aVL, II and aVF. With multi-lead STD, there is of course STE in aVR.
This pattern and location of STD (maximal in V1-V4) is indicative of focal, posterior transmural infarction, with the most likely etiology being Occlusion MI. Notably, this is NOT the pattern of diffuse supply/demand mismatch, in which the STD is maximal in V4-6 and lead II.
There are other possibilities, such as a "type II STEMI", for example: acutely increased demand (in this case due to rapid ventricular response) on an already chronically stenosed LCX, resulting in massive supply/demand mismatch and transmural ischemia. But this would be a diagnosis of exclusion compared to the possibility of OMI, given the diagnostic ECG.
Back to the case:
The first troponin T was negative (less than 0.01 ng/mL) and the patient was admitted to the cardiology unit.
The second troponin T returned at 0.20 ng/mL and a repeat ECG was ordered at around 8 hours after presentation:
The patient has converted back to sinus rhythm. Still slight STD in V3-V5, but otherwise the findings of OMI are much improved compared to the initial ECG. We do not know if the patient still had active pain at this time, but I would suspect that this ECG represents reperfusion (or collateral circulation).
Troponins continued to rise with peak 0.67 ng/mL at about 24 hours from presentation. Echo showed moderated to severe mid to basal inferolateral wall hypokinesis (What is commonly referred to as the posterior wall). Apparently at this time the patient was no longer symptomatic, so cath was scheduled for the next morning.
The cath showed a complete thrombotic occlusion of the LCX (collateral flow was not commented on, but could have been present). The LCX was stented open with good angiographic result. There was also other chronic CAD in various vessels without any other acute culprits.
Here is the post-cath ECG:

Roughly the same as before the cath.
The patient did well.
Learning Points:
When there are multiple leads with STD, then you must find where the STD is maximal. STD maximal in V1-V4 is posterior OMI until proven otherwise. Diffuse supply/demand mismatch ischemia presents with STD maximal in V4-V6 and lead II (the average overall axis of depolarization), and therefore must always also present with STE in aVR.
See this diagram that highlights this learning point:

When ECG findings of OMI are present in the setting of AF with RVR, one of the initial steps in management is to control the rate which will reduce supply demand mismatch and allow for a repeat ECG at reduced heart rate (with better quality and the chance to see if the ischemic findings have resolved with reduced rate).
See this similar case:
Steve and Pendel...
ReplyDeleteThanks for an excellent case with lots of teaching points. Ken hasn't posted yet and I know he will have lots to say. This is one of those cases in which the LCx as the culprit artery should come as no surprise if you know your anatomy. Here are my thoughts...
First, one must realize that there are TWO possible RCA's, TWO possible LCx's and THREE possible LAD's: The RCA and LCx both have dominant and non-dominant forms and the LAD has a Type 1, Type 2 and Type 3. It's easy to start narrowing down the culprit artery: only two coronary arteries will cause ischemic depression limited to V1 - V4 (which is actually reciprocal depression). Of course, LAD stenosis could also do that, but it is usually associated with ST depression in other leads as well. And LAD occlusion would be much more likely to result in STE in those leads. So, we will limit our diff dx here to an OMI of the RCA and the LCx.
A posterior (or lateral or posterolateral) epicardial ischemia caused by the RCA typically represents an occlusion of the posterolateral branch (PL) which is the LAST branch of the RCA. The PL is the continuation of the RCA AFTER the posterior descending artery (PDA). While it is quite common for a distal occlusion to include both those arteries, it would be extremely rare for an occlusion to involve ONLY the PL.
With the LCx, the PDA branches well AFTER the PL. Now remember that while an RCA occlusion PROXIMAL to the PDA will almost always involve the PL as well, the LCx is going to be supplying that area also - even when non-dominant. So many distal occlusions of the RCA do not result in STD in V1 - V3/4 because the LCx may also be providing that area with circulation - again, even when non-dominant.
About 80% - 85% of the time, however, the LCx is non-dominant which means a distal occlusion will only involve the PL branch causing STD in V1 - V3/4. That's why OMI with isolated STD in V1 - V3/4 is more typically caused by an LCx occlusion and not the RCA. Obviously, in those cases the PL branch from the RCA is unable to provide sufficient circulation to prevent the ischemia.
However, I think it is likely that this was a PROXIMAL occlusion of the LCX. This would also involve the obtuse marginals and the posterolateral branches but, more importantly, it would also involve the artery to the SA node which, when present, is located very proximally on the LCx. There is also a proximally-located SA nodal artery on the RCA but most people don't know about the one on the LCx. And, unlike the artery to the AV node whose presence depends on arterial dominance, the SA nodal artery occurs on the LCx 45% of the time REGARDLESS of dominance. The SA nodal artery exists on EITHER the RCA OR the LCx - but very, very RARELY on both so only ONE of those arteries controls the circulation to the SA node and 45% of the time it's the LCx. This loss of circulation has likely contributed to the atrial fibrillation. We don't see other evidence of basolateral or apicolateral ischemia because the LAD, a possible ramus intermedius and perhaps even the RCA also supply those areas.
Thus we can see why there is STD in V1 - V4, no inferior STE, no significant basolateral or apicolateral ischemia and the onset of atrial fibrillation - all caused by a single proximal occlusion of the LCx. I realize there is a small amount of STD in V5 also, but I think that relates more to the loss of circulation from the obtuse marginals. In theory, if the LCx were dominant, such a proximal occlusion could result in simultaneous acute epicardial ischemias of the basolateral and inferior walls with cancellation of all opposing forces on the ECG tracing. However, this was not supported by the echo.
Thanks for a great case!
THANKS so much Jerry! Your detailed comment is a lesson in coronary anatomy! — :)
DeleteVery interesting case,thanks a lot.
ReplyDeleteOur pleasure! — :)
DeleteThere is subtle STE in III and V6, - I would have written "Posterior STEMI" in this case.
ReplyDelete@ Max — I do NOT believe ( = my opinion) that ST segments in lead III and in lead V6 consistently show ST elevation. As per Dr. Meyers — it is the fact that there is clearly MORE ST depression in leads V2-thru-V4 (compared to the relative amount of ST depression in other leads) that suggests there may be acute posterior OMI in this case. I do NOT think this localization to the posterior wall is 100% predictive ( = my opinion) — because there IS substantial tachycardia + some ST depression in virtually all other leads — but I agree completely with Dr. Meyers that acute posterior OMI does need to be considered until it can be proved otherwise. THANKS for your comment — :)
DeleteHad a fairly similar one last week, woman in her mid-80's. She had even more impressive STD's (like 3mm) but her heart rate was nearly 180 (and very regular). I was fairly uncertain on initial evaluation as her chief complaint was severe chest pain and she had a BP of 70/50 and she literally looked like she was dying and I wasn't sure if it was cardiogenic shock and compensatory tachycardia or simply unstable.
ReplyDeleteFortunately she converted abruptly in front of me to a more irregular AFib with RVR in the 120's and a much improved pressure and complete, and abrupt, resolution of her chest pain.
In retrospect, she was fairly obviously in either Atrial Flutter/Fib with demand ischemia rather than an overt occlusion. I really got thrown by clinically how much pain she was in. The rate was just too fast for a sinus tachycardia at that age.
Anyway, thanks for sharing, my case has been on my mind this week.
THANKS for your comment Dan! Reasons new-onset rapid AFib is so commonly associated with acute coronary insufficiency/heart failure include: i) Loss of the “atrial kick” (which typically provides between 5-40% of cardiac output — but much closer to the HIGHER range in older women who are the most prone to longstanding hypertension + resultant diastolic dysfunction that leads to greater dependence on atrial “kick” for cardiac filling); and ii) The rapid rate of the AFib — with ANY tachycardia dysproportionately shortening the period of diastolic filling more than systole — such that ANY tachycardia tends to reduce cardiac output. So, tachycardia (esp. from new, rapid AFib) is a common cause of diffuse subendocardial ischemia in elderly subjects — and sometimes you won’t know how much of the hypotension, chest pain/ischemia, poor perfusion will resolve once the patient is converted out of AFib, and back to a reasonable heart rate …
Deleteextraordinary. thank you docs T,P and S. what i find most frightening is how much i don't know... i should have known about the above, and didn't till now.
ReplyDeletethank you.
Thanks Tom! We are ALL learning every day! Cases like this are great to facilitate that learning — :)
Delete