
This was sent to me by John Larkin, from Australia, who has a great ECG Blog called "ECG of the Week," where he posted it, and graciously allowed me to post it here.
The ECG is from an elderly male with multiple co-morbidities including significant cognitive impairment, cardiac failure and diabetes. He presented to the Emergency Department with several hours of chest pain and has a pacemaker in-situ for an unknown indication.
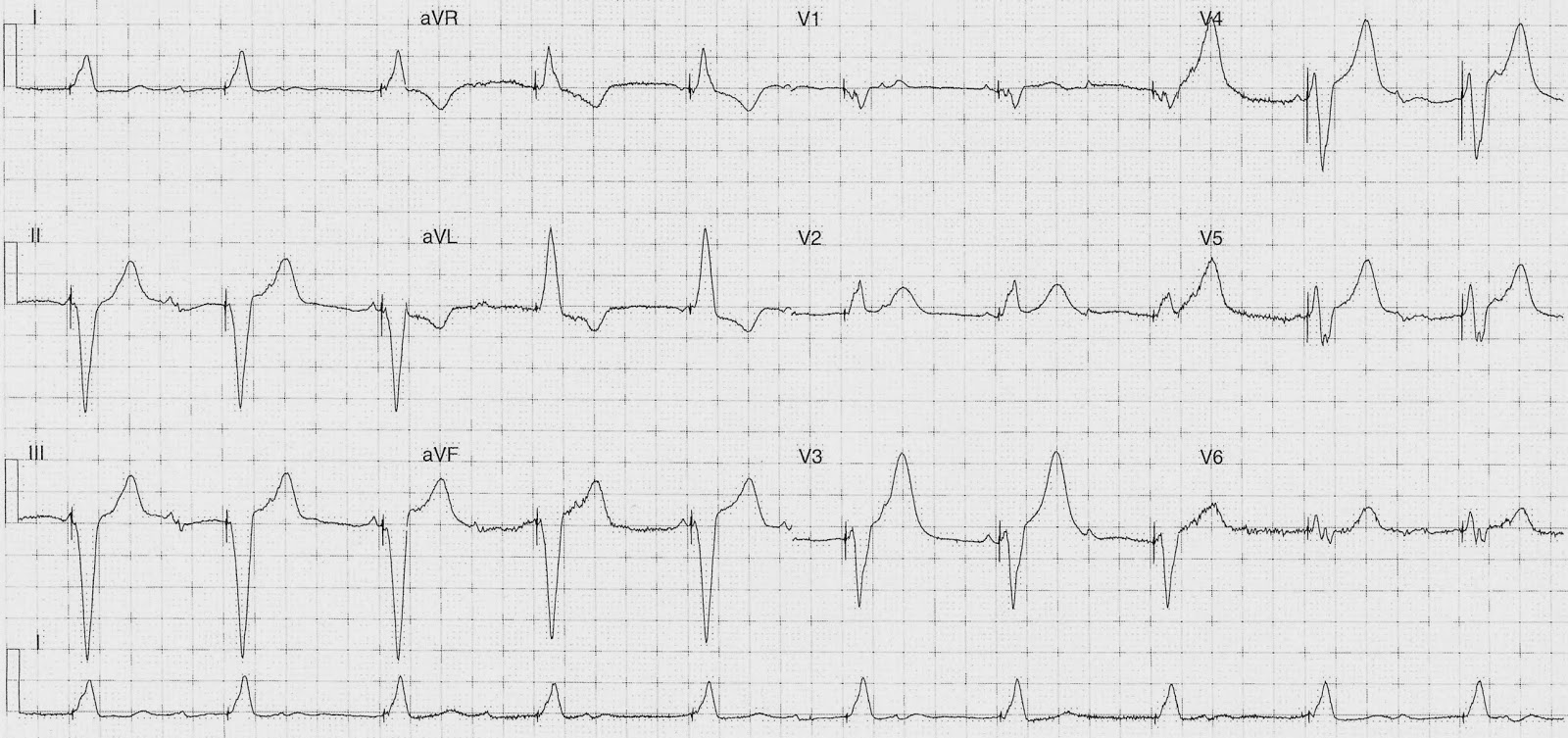
Here is his ECG:
John's thoughts on the ECG are as follows:
· Regular V-paced rhythm at 60 bpm with LAD.
· Lead V2 has concordant ST elevation but less than 1mm
· Lead V3 has excessive discordant ST elevation (ratio -0.33)
· Lead V4 has excessive discordant ST elevation (ratio -0.32)
· Lead V5 I suspect has excessive discordance but the baseline wander and native P wave superimposition makes it difficult to measure
· The T waves in leads V2-6 are huge compared with the QRS voltages
· Evidence of non-conducted native atrial activity
My thoughts
I was less certain of LAD occlusion because of the profound upward concavity, and I didn't think any lead met a consistent ratio of 0.25, though I think V3 did meet a ratio of 0.20. But was very suspicious of the very large T-waves.
One should keep in mind that in our LBBB studies (we have two now, with data forthcoming on the second, and larger, validation study) an ST/S ratio of 0.20 is more sensitive though slightly less specific, than 0.25.
But a ratio of 0.20 is still nearly 90% specific.
All this data is for LBBB and I do believe that it applies to paced rhythm.
Follow-up
The patient was not taken for angio given their extensive co-morbidities (including GI bleed) following discussion with both cardiology and patient’s family. He did have a troponin rise and was treated with maximal medical therapy.
Although he did not have an angiogram, followup ECGs, echos, and troponin prove that he did, indeed, have an LAD occlusion.
His initial troponin I was 6.7 ng/mL.
Echo showed EF of 30% with large amount of severe segmental systolic dysfunction.
This was 130 minutes later:
 |
| Now lead V4 has a ratio of 0.25 |
This was recorded at 6 hours:
 |
| The hyperacute T-waves are gone. The ST segments have nearly resolved. |
This one is at 20 hours
 |
| Still more resolution of ST elevation and T-waves |
 |
| T-wave starting to invert |
In some data we have recently collected and will publish, we have shown that reperfusion of an occluded artery in LBBB, just like in normal conduction, results in reperfusion T-waves in many, if not most, cases.
Is this also true in paced rhythm?
This one is at 43 hours
 |
| More T-wave Inversion (reperfusion T-waves vs. evolution of completed MI) |
345 hours
 | |
|
454 hours
 |
| T-waves are deeper still |
Learning Points
1. Hyperacute T-waves may be seen in paced rhythm
2. The Modified Sgarbossa criteria are likely applicable in paced rhythm as well as in LBBB
3. The ECG often evolves T-wave inversion in reperfusion of an occluded artery in both LBBB and in Paced rhythm.
Very nice series of tracings showing evolutionary changes of a stemi in a patient with a pacemaker. The images to “engrain” in one’s mind are comparison of the ST-T waves seen in the initial paced-rhythm ECG - compared to the ECG at 20 hours. THANKS to Drs. John Larkin & Steve Smith for posting this interesting case!
ReplyDeleteThanks, Ken!
DeleteNice
DeleteThe evolution of the reperfusion T waves in the serial ECGs look similar to the evolution of Wellens T waves. As far as I understand the mecanism is similar; how can we distinguish between them?
ReplyDeleteThat is exactly what they are. No need to distinguish because they represent the same pathology.
Delete