
A 30 year old collapsed after complaining of chest pain intermittently. He was unconscious. First responders thought they palpated a thready pulse.
When medics arrived, there was no pulse. Full CPR was initiated with the LUCAS device. The patient was intubated, an ITD (ResQPod) was used. Other standard cardiac arrest measures were undertaken.
Here is the rhythm strip (these are two separate tracings):
The patient could not be resuscitated, but was transported to the ED after about 30 minutes of full arrest.
Upon arrival, as is customary, a very brief ultrasound was performed to assess ventricular function.
What do you see? See below, with arrows
Here is one more brief view before chest compressions resumed:
When medics arrived, there was no pulse. Full CPR was initiated with the LUCAS device. The patient was intubated, an ITD (ResQPod) was used. Other standard cardiac arrest measures were undertaken.
Here is the rhythm strip (these are two separate tracings):
 |
| The initial rhythm is regular and wide complex, with concordant ST elevation, suggesting STEMI. The next rhythm appears to be ventricular fibrillation. |
The patient could not be resuscitated, but was transported to the ED after about 30 minutes of full arrest.
Upon arrival, as is customary, a very brief ultrasound was performed to assess ventricular function.
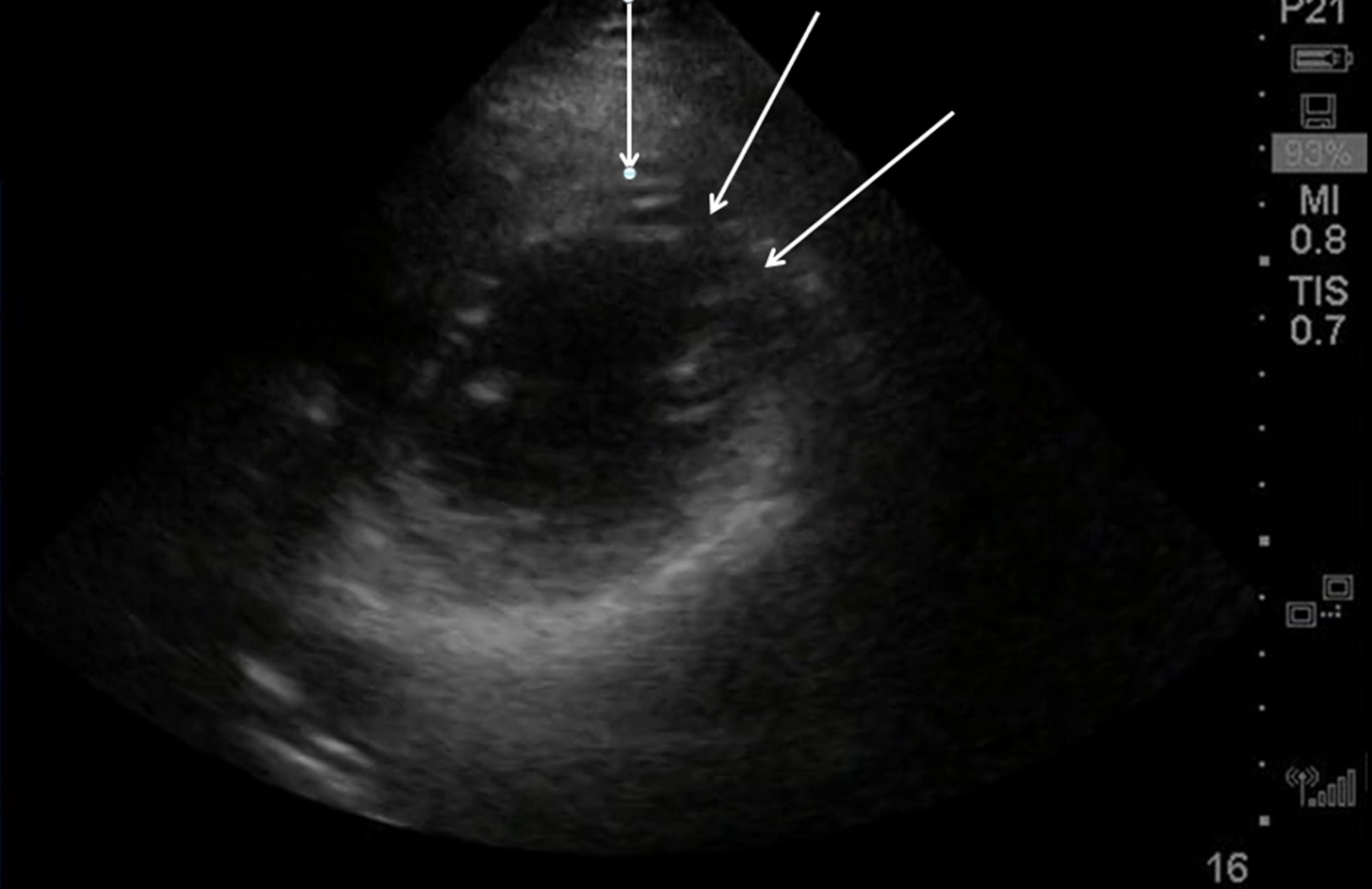
What do you see? See below, with arrows
 |
| White arrows outline a very large thrombus (clot) in the pericardium. Red arrow points to a small amount of liquid blood in the pericardium. Blue arrow points to the RV, where there is full stasis of blood flow. Green arrow points to barely beating LV |
Here is one more brief view before chest compressions resumed:
Here is a view during LUCAS chest compressions
Of course, chest compressions are not of any use when there is massive tamponade. Even when the heart is fully beating on its own, it will arrest if there is severe tamponade because it cannot generate adequate pressures for myocardial perfusion. So how would external compressions have any effect?
For cardiac compression to work, the clot must be evacuated.
Although there seemed little hope of recovery, a left thoracotomay was quickly performed. A pericardiotomy was performed and this clot was evacuated:
 |
| Huge clot extracted from pericardium. This is about 30 cm x 15 cm on the cart. |
In spite of internal cardiac compressions, intracardiac epinephrine, several internal defibrillations for V fib, and other standard attempts at resuscitation, he could not be resuscitated. The resuscitation was futile.
What caused this hemopericardium?
Possible etiologies include:
1. Hemorrhagic pericarditis, but this would be mostly effusion with some blood, not hemopericardium and certainly not clotted blood.
2. Myocardial rupture from MI.
3. Myocardial rupture from trauma (could be occult, could be due to chest compressions)
4. Ruptured coronary artery aneurysm
Here is an ED ultrasound of the aorta through the suprasternal notch:
This is annotated with arrows below:
 |
| These arrows point to a flap. This is aortic dissection. The aortic diameter is also excessive (greater than 4 cm is abnormal, here it is about 6 cm) |
Autopsy showed a DeBakey 1 dissection ( from the arch all the way to the iliac bifurcation)
Thus, this unfortunate young man had an aortic dissection at a very young age. It dissected back into his pericardium, resulting in hemopericardium and tamponade, which caused hemodynamic collapse. His pulses by first responders were thready, but not enough to perfuse his brain. Thus he was unconscious. Shortly thereafter, the hypotension with consequent poor perfusion of his coronary arteries resulted in severe ischemia with transmural/subepicardial ischemia, and a wide complex then eventually ventricular fibrillation.
Causes of Pulseless Electrical Activity (5 H's and 5 T's), as advertised by ACLS
Those bolded are particularly likely with a narrow QRS
Hypovolemia
Hypoxia
Hydrogen ions (acidosis)
Hyper/Hypokalemia
Hypo/Hyperglycemia
Tamponade
Toxins
Tension Pneumothorax
Thrombosis (myocardial infarction)
Thromboembolism (Pulmonary embolism)
Was there any chance of resuscitation with thoracotomy? Probably not, but worth a try.
Once there is full arrest from tamponade, and it has been ongoing for this long, I believe that resuscitation is futile. However, with a health 30 year old, one must try.
Here is a case in which the patient was alive in the ED and then arrested, had a thoracotomy (in this case subxiphoid) and survived. The blood was not clotted.
In contrast, in this study of out of hospital cardiac arrest from non-traumatic pericardial fluid on ultrasound, only 1 of 23 patients survived. None had dissection and none had clotted blood on hemopericardium. The survivor had liquid blood from myocardial rupture.
Here is a case of myocardial rupture.
Here is another case of myocardial rupture.
Here is a great published case series of myocardial rupture, by my colleague Dave Plummer. Plummer D et al. Emergency Department Two-Dimensional Echocardiography in the Diagnosis of Nontraumatic Cardiac Rupture. Annals of EM 23(6):1333-1342; June 1994. All of these patients had ECGs with ST elevation, but ultrasound showed pericardial fluid (not clot) and the patient had MI with rupture.























{kind=link}