
This case comes from Jason Winter, of The Facebook Clinical Electrocardiology ECG Page.
A 60-something woman called EMS for chest pain.
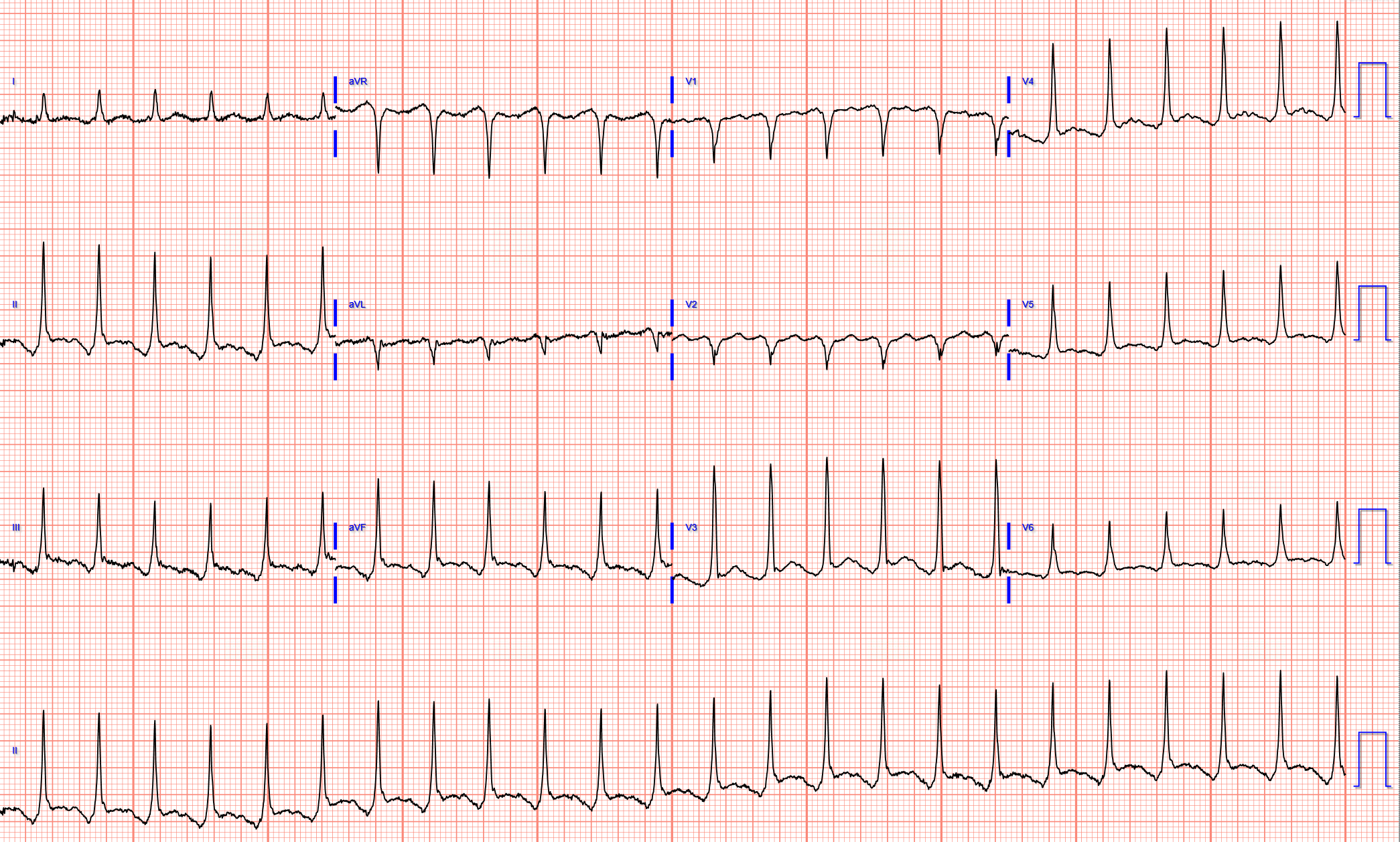
Here is her first prehospital ECG:
There is very low voltage in the precordial leads, with a total QRS amplitude of only 3.5 mm in V2 and 4 mm in V3.
In spite of this low voltage, there is ST elevation (as measured at the J-point and relative to the PQ junction, and as measured by the computer and shown on the right), of 0.54 mm in V2 and 0.65 mm in V3.
The ST/QRS ratios in V2 and V3 are, respectively, 0.154 and 0.162. These are a high ST/QRS ratios.
In our study of subtle LAD occlusion vs. early repolarization, the mean ratio of ST/QRS was:
-- 0.215 and 0.195 for V2 and V3 in LAD occlusion vs.
-- 0.077 and 0.081 for V2 and V3 in early repolarization.
The specificity of a value in V2 greater than or equal to 0.154 was 90% (90 of 100 cases).
The specificity of a value in V3 greater than or equal to 0.162 was 84% (79 of 94 cases).
However, we did not include cases with less than 1 mm of ST elevation, so strictly speaking, one should be circumspect about applying such ratios. Nevertheless, these high ratios certainly suggest that there is abnormal ST elevation in the leads of the LAD territory.
How about if we apply the LAD occlusion/early repol formula?
STE60V3 = 1
QTc = 397
RAV4 = 0.5
This produces a value of 24.46 (greater than 23.4 is nearly diagnostic of LAD occlusion). However, again, the formula was developed only in ECGs with at lead 1 mm of STE in V2 and V3, so does it apply?
Here is the same ECG stretched vertically so that the QRS amplitude is closer to normal:
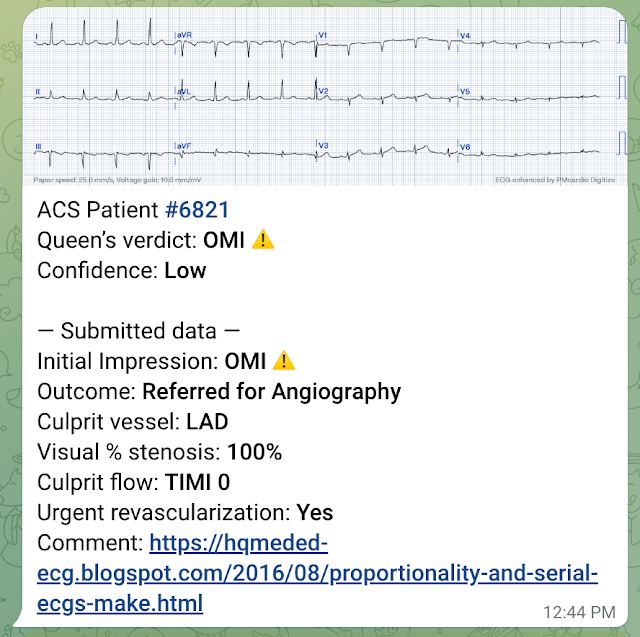
I sent this to the Queen of Hearts PMCardio AI app and the Queen diagnosed it (but with low confidence).
A 60-something woman called EMS for chest pain.
Here is her first prehospital ECG:
 | |
|
There is very low voltage in the precordial leads, with a total QRS amplitude of only 3.5 mm in V2 and 4 mm in V3.
In spite of this low voltage, there is ST elevation (as measured at the J-point and relative to the PQ junction, and as measured by the computer and shown on the right), of 0.54 mm in V2 and 0.65 mm in V3.
The ST/QRS ratios in V2 and V3 are, respectively, 0.154 and 0.162. These are a high ST/QRS ratios.
In our study of subtle LAD occlusion vs. early repolarization, the mean ratio of ST/QRS was:
-- 0.215 and 0.195 for V2 and V3 in LAD occlusion vs.
-- 0.077 and 0.081 for V2 and V3 in early repolarization.
The specificity of a value in V2 greater than or equal to 0.154 was 90% (90 of 100 cases).
The specificity of a value in V3 greater than or equal to 0.162 was 84% (79 of 94 cases).
However, we did not include cases with less than 1 mm of ST elevation, so strictly speaking, one should be circumspect about applying such ratios. Nevertheless, these high ratios certainly suggest that there is abnormal ST elevation in the leads of the LAD territory.
How about if we apply the LAD occlusion/early repol formula?
STE60V3 = 1
QTc = 397
RAV4 = 0.5
This produces a value of 24.46 (greater than 23.4 is nearly diagnostic of LAD occlusion). However, again, the formula was developed only in ECGs with at lead 1 mm of STE in V2 and V3, so does it apply?
Here is the same ECG stretched vertically so that the QRS amplitude is closer to normal:
 |
| Now one can appreciate the ST elevation a bit better. |
I sent this to the Queen of Hearts PMCardio AI app and the Queen diagnosed it (but with low confidence).

YOU TOO CAN HAVE THE PM Cardio AI BOT!! (THE PM CARDIO OMI AI APP)
If you want this bot to help you make the early diagnosis of OMI and save your patient and his/her myocardium, you can sign up to get an early beta version of the bot here. It is not yet available, but this is your way to get on the list.
Clinical Course
I don't know if the medics noticed these ECG findings or not, but if not, they recognized the value of serial ECGs in a patient with chest pain.
Here are these serial ECGs, starting with the first one again:
#1: Time zero:
#2: 27 seconds later:
#3: 74 seconds after #2
#4: 56 seconds after #3: [157 seconds (2 min 37 sec) after the first]:
The medics administered aspirin (no Nitroglycerine), and the pain resolved.
#5: 18 minutes after #4:
#6: 4 minutes after #5:
Case Outcome
Because of ST resolution, the patient was not taken that night to the cath lab. She was treated for NonSTEMI with antiplatelet and antithrombotic agents and went to cath the next day, where an where multiple LAD thrombi were found and the lesion will be stented.
Waiting to cath a transient STEMI can be hazardous. See this case in which I made that mistake.
Learning Points:
1. Repolarization (ST-T) is proportional to depolarization. All ST elevation (and T-wave size) should be assessed relative the QRS amplitude.
2. Serial ECGs improve the sensitivity of ST elevation on the ECG for MI. In the only ED study of its kind, sensitivity increased from 46% to 62%.
I don't know if the medics noticed these ECG findings or not, but if not, they recognized the value of serial ECGs in a patient with chest pain.
Here are these serial ECGs, starting with the first one again:
#1: Time zero:
 | |
|
 | |
|
 | |
|
 | |
|
The medics administered aspirin (no Nitroglycerine), and the pain resolved.
#5: 18 minutes after #4:
 | |
|
 | |
|
Because of ST resolution, the patient was not taken that night to the cath lab. She was treated for NonSTEMI with antiplatelet and antithrombotic agents and went to cath the next day, where an where multiple LAD thrombi were found and the lesion will be stented.
Waiting to cath a transient STEMI can be hazardous. See this case in which I made that mistake.
Learning Points:
1. Repolarization (ST-T) is proportional to depolarization. All ST elevation (and T-wave size) should be assessed relative the QRS amplitude.
2. Serial ECGs improve the sensitivity of ST elevation on the ECG for MI. In the only ED study of its kind, sensitivity increased from 46% to 62%.
Here they all are together:








-USE.png)
-USE.png)






-USE.png)