
This history and ECG were texted to me from a far away ED on a Friday night:
"Very elderly make with history of coronary disease on an angiogram 1 year prior presents with 2 hours of chest pain, sternal, pressure, and mild diaphoresis."
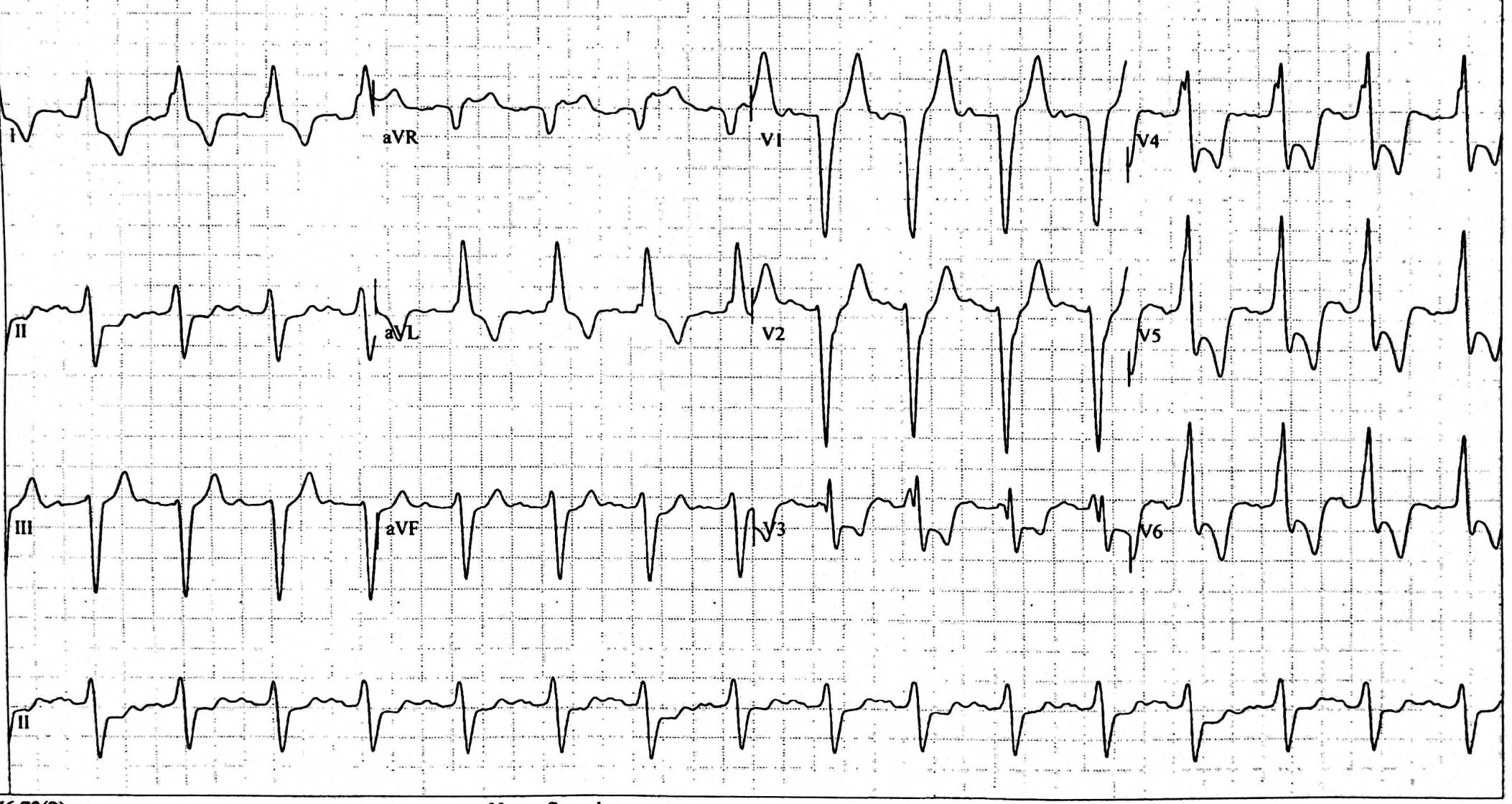
There is sinus tachycardia with LBBB. There is concordant ST depression (STD) in lead V2, and excessively proportionally discordant STD in all of leads V3-V6. Thus, there is one lead (V2) that meets the Sgarbossa criteria and the Smith modified criteria, and 4 other leads (V3-V6) that meet the alternative Smith modified criteria (proportionally excessively discordant ST depression at an ST/R ratio >0.30).
Additionally, there is ST Elevation in aVR. The ECG is low resolution and so it is difficult to determine the exact measurements, but I believe it measures at 1.5 mm. The S-wave is 3.0 mm, and so this lead ALSO meets the Smith Modified Sgargossa criteria. So the criteria are met in 6 leads, when only one is necessary!! In both of our studies of the Modified Sgarbossa criteria, not only was the presence of the criteria in just one lead much better than the original Sgarbossa criteria, but the proportionally excessively discordant findings were present in far more leads than in the Original criteria, and so it was more visually obvious and stunning.
In the case, the maximal ST depression is in lead V4, both in an absolute millimeter measurement and as a proportion to the preceding R-wave amplitude. Whether normal conduction or LBBB, STD maximal in V1-V4 is very specific for posterior OMI, whereas V5-V6 is typical of non-occlusive but obstructive ischemia.
In either case, cath lab activation is indicated!!
The physician who sent this tried to transfer the patient to an interventional center, but initially failed.
He wrote: "I'm going to try interventional cardiologist at XXXXXX as the cardiologist at the first hospital was not impressed."
So he called the interventional cardiologist at the other receiving center, and this was the response: "Interventional cardiologist at YYYYYY said that is is not a real STEMI."
I told him: "Send the patient!! Do not take "no" for an answer!!"
And so he did. And forced their hand.
Subsequent events
When the patient arrived, the troponin (not high sensitivity) was 29.4 ng/mL (very high, typical of large STEMI). On arrival, the symptoms were improved, but we do not have another ECG to see if it, too, is improved.
At angiogram, they found this:


In our validation study of the Smith Modified Sgarbossa criteria, we identified 4 patients who did not meet our definition of ACO yet did have notable catheterization findings and outcomes warranting immediate diagnosis and intervention. These 4 patients were found to have AMI and new 3-vessel or left main coronary artery disease with either 1) an acute but non-occlusive culprit lesion, or 2) very high troponin. Peak 24-hour troponin T levels were 0.25, 0.75, 1.04, and 6.61 ng/mL. Two of these 4 required urgent or emergent coronary artery bypass graft. We categorized these patients as having “acute 3-vessel/left main disease myocardial infarction” (3V/LMD). Three of these 4 patients had discordant ST elevation (STE/S ratio > 20% in lead aVR), but only 1 of these 3 was positive by the 25% modified criteria. Two of the four 3 V/LMD patients also met the ST depression criteria (ST Depression to R-wave > 30%) due to widespread ST depression in various other leads, including III, aVF, V5, and V6. None of the 4 met the weighted or unweighted original Sgarbossa criteria. If “new 3V/LMD” (without a specific culprit lesion identified) had been classified as equivalent to a culprit lesion in our definition of ACO, the sensitivity of each rule would be reduced by 1% to 3%, and specificity would remain unchanged, but more patients with potential need for urgent revascularization would have been identified.
Learning Points:
1. Formerly, it was thought that myocardial infarction (MI) could not be diagnosed in LBBB. "MI" formerly meant "Old MI" as represented by Q waves. "Acute transmural ischemia" is different from "MI". In fact, infarction is the end result of completed transmural ischemia.
2. The STEMI criteria used in normal conduction (absence of BBB) are NOT very sensitive for Acute Transmural Ischemia (OMI) because they do not use proportionality or any other features of acute ischemia other than a fixed millimeter amount of ST Elevation.
In fact, the Smith Modified Sgarbossa criteria in LBBB are far more sensitive for OMI than are the STEMI criteria in normal conduction!!! This is because they use proportionality and because, contrary to conventional wisdom, LBBB does NOT hide transmural ischemia if you use proportions.

- When acute ECG changes in a patient with LBBB are subtle — diagnostic aids such as Smith-modified-Sgarbossa criteria may be helpful. At other times (such as for the ECG in Figure-1) — the diagnosis of an acute cardiac event is obvious, even without the need to invoke modified Smith-Sgarbossa criteria.
-USE.png) |
| Figure-1: The initial ECG in today's case. |
- In addition to use of Smith-modified-Sgarbossa criteria — I routinely favor a qualitative approach. Realizing that conduction defects (LBBB, RBBB, IVCD) and ventricular pacing may each alter expected ST-T wave appearance — I look for those leads that clearly show ST-T wave findings that should not be there.
- Among the flagrant ST-T wave changes in Figure-1 that should be immediately apparent — the ST segment coving and huge amount of J-point ST depression (that exceeds 5 mm in lead V4!) — in this elderly patient with new-onset chest pain — should prompt the need for immediate cath without having to delay for additional data.
- For typical LBBB — there should be predominant negativity (ie, no more than a tiny initial r wave) in right-sided lead V1 — as well as in other anterior leads. The fact that a significant R wave is already present in lead V3 is not expected with a "typical" LBBB.
- Looking closer at QRS morphology in lead V3 — there is alternation for the 4 beats seen in this lead between a qRS pattern (for the 1st and 3rd beats in this lead) — with a "fat" initial R-slur-R'-S for the 2nd and 4th beats in this lead. This is bizarre. It doesn't seem to be artifact. If "true" QRS morphology in lead V3 is the qRS pattern — then this initial q wave is abnormal and suggestive of infarction. If instead the R-slur-R'-S pattern is the "true" morphology — then this is marked fragmentation, consistent with "scar" from underlying heart disease.
- In left-sided leads with typical LBBB morphology — there should be a monophasic (all upright) R wave. We see this in leads I and aVL — but there is a fairly deep S wave (of 5 mm) in lead V6. While true that many patients with LBBB and LVH only develop a monophasic R wave in more laterally placed leads (such as lead V7 or V8) — awareness that QRS morphology is indeed somewhat atypical for LBBB is relevant for helping us to interpret the significance of ST-T wave changes. There is simply no way that the ST segment coving in leads V3-thru-V6 could be "normal" (not to mention the huge inappropriate amount of ST depression).
- BOTTOM Line: As per Dr. Smith — this elderly man with new-onset chest pain should have been accepted for immediate cath on the basis of his initial ECG.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.