
Written by Pendell Meyers
A man in his late 40s with several CAD risk factors presented with acute chest pain. He had several episodes lasting several hours over the past few days, with a more intense episode starting 1 hour prior to arrival. He described the pain as substernal squeezing and nonradiating, and associated with diaphoresis. He had some recent cocaine use 3 days ago.
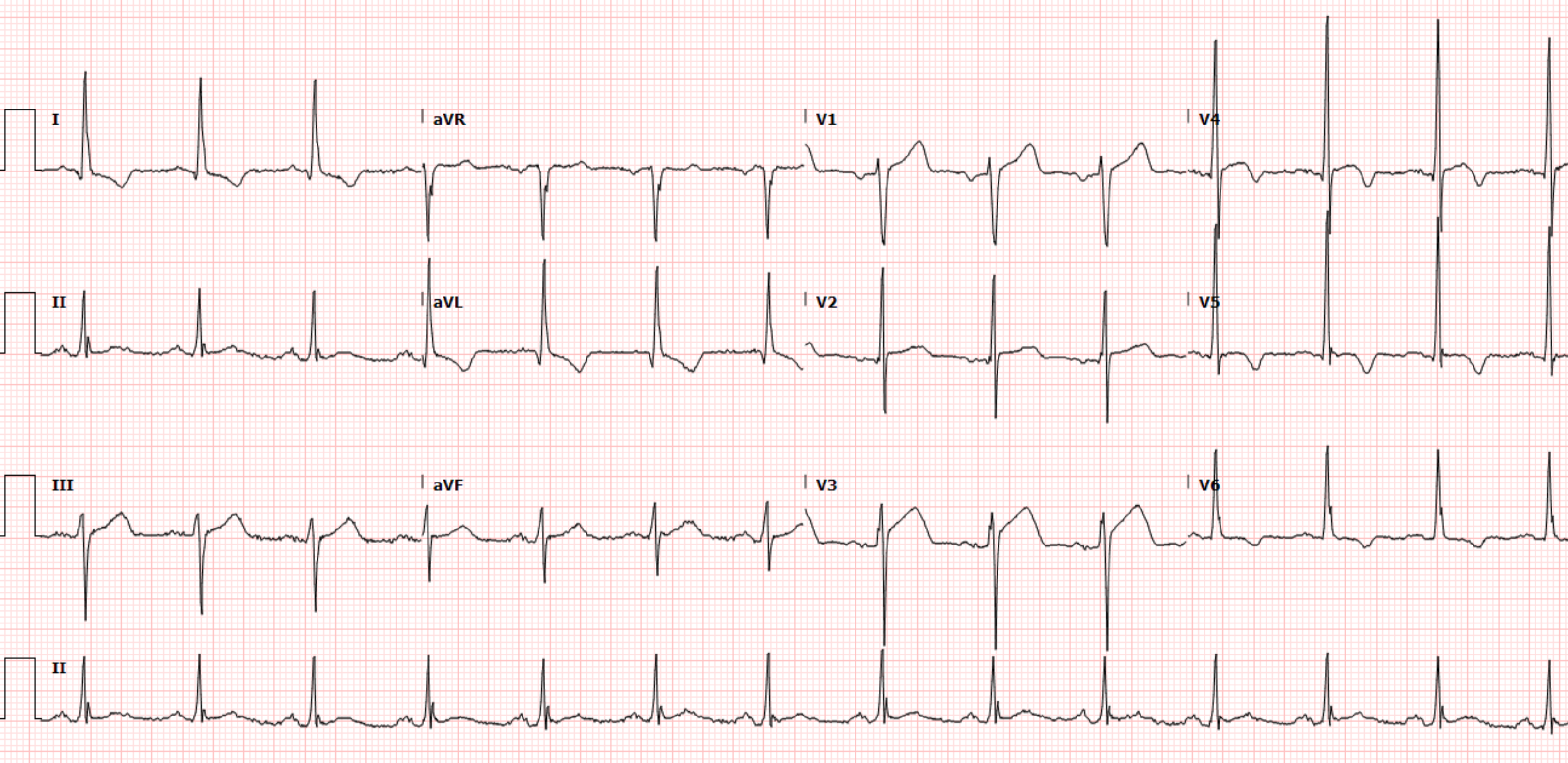
Here is his triage ECG:




Repeat troponins:
39 ng/L
40 ng/L
40 ng/L
39 ng/L
Echo:
Moderate concentric LV hypertrophy
EF 61%
No segmental wall motion abnormalities
No pericardial effusion
The medicine team consulted cardiology, who advised that no further workup was indicated at this time. They referred to a coronary CT angio performed about 1 year ago which showed several coronary arteries with nonobstructive CAD. Somehow this was used as part of the reasoning not to perform further workup.
No definitive cause of chest pain was found. The discharge note described possible musculoskeletal, esophageal, and cocaine-related causes as possibilities.
Learning Points:
Abnormal depolarization usually results in abnormal repolarization, and learning the expected repolarization patterns is critical for improving diagnostic performance in ECG interpretation.
LVH produces some of the most difficult STEMI and OMI mimics out there.
OMI is not just an ECG diagnosis.
We must focus on learning false positive ECG patterns in parallel with learning the false negative STEMI(-) OMI patterns.

- Most of the time (as was true for today's case) — a single ECG will not suffice for telling you if the cath lab needs to be immediately activated. Instead — comparison with prior and/or serial tracings + troponins (and optimally stat Echo) — will be needed for optimal decision-making.
- For clarity — I've reproduced the initial ECG in Figure-1.
-USE%20copy.png) |
| Figure-1: The initial ECG in today's case. |
- Small and narrow q waves are seen in leads I, aVL; V4 and V5 — but strangely enough, not in lead V6. That said — I still suspect these are normal septal q waves.
- Criteria for LVH are easily satisfied in multiple leads (ie, very tall R in aVL ~14 mm; very tall R in V5 22 mm + S in V1 >35 mm). For "My Take" on a user-friendly approach to the ECG diagnosis of LVH — See My Comments in the June 20, 2020 and April 27, 2019 posts in Dr. Smith's ECG Blog.
- ST-T wave changes in high-lateral leads I and aVL look completely typical for LV "strain" — because there is no more than minimal J-point depression with a slow downslope to the ST segment, followed by a more rapid upslope. The amount of ST-T wave depression in these leads is perfectly proportional to what I'd expect given the R wave amplitude in these same leads.
- In contrast — the ST-T wave changes in lateral chest leads V5 and V6 look different. That is, the ST segment is flat — and the T waves are symmetrically inverted, consistent with either LV "strain" and/or ischemia. That said, the important point given this patient's presentation to the ED with new chest pain — is that nothing I've described thus far suggests acute OMI or the need for immediate cath.
- Given modest depth of the S wave in lead V3 — the reason for my concern was that I thought the amount of J-point ST elevation in this lead V3 was more than I'd expect for the anterior ST elevation sometimes seen with LVH.
- I suspected the ST-T wave appearance in lead V4 represented a transition between the positive ST-T wave of lead V3 — and the T wave inversion of lead V5. That said — the ST segment in lead V4 was clearly coved, so I thought it impossible to say that this was not acute.
- To Summarize: The patient in today's case presented with new-onset chest pain. While I was not at all convinced that ECG #1 represented an ongoing acute process — I felt there was no denying that: i) Lead V3 could represent a hyperacute ST-T wave; ii) If lead V3 did represent a hyperacute ST-T wave — then the ST segment coving in lead V4 could be the tail end of this process; iii) While not necessarily abnormal taken by itself — the ST-T wave in lead V1 was clearly taller than is usually seen in this lead; and, iv) I had no doubt that lead V2 was malpositioned.
- Given i), ii) and iii) in the above bullet Summary — I felt the "true" appearance of lead V2 was essential for accurate interpretation of this initial ECG. Therefore — I would have verified lead placement — and immediately repeated the initial ECG on this patient.
- Of note — R wave progression was normal on the baseline ECG done 1 year earlier (ie, the 2nd ECG shown above in this case).
- After pain resolution in the ED — the ECG was repeated. This is the 3rd ECG shown above in today's case — and it once again strongly suggests malposition of lead V2 (once again rendering this lead useless in our interpretation). Since this repeat ECG was recorded in the ED not long after the initial tracing — I suspect that the same technician (who was responsible for malposition of lead V2 in the initial tracing) — was probably also the one to record this repeat ECG after chest pain resolved.
- Later that day — and again on the next day — a 4th and 5th ECG was obtained. Both of these last 2 tracings showed normal R wave progression. Since these tracings were done presumably hours (or more) after the first 2 ECGs — presumably a different technician recorded these tracings (which is why I suspect that R wave progression is now normal).
- In Conclusion: Whereas I did not feel we could rule out an OMI from the initial tracing shown in Figure-1 — none of the subsequent tracings in today's case were suggestive of an acute event. I suspect that IF the initial ECG would have been immediately repeated with accurate chest lead electrode placement — that there may not have been any need for concern about a possible acute event from the initial ECG.
- Learning Point: When clinical decision-making hangs in the balance and you strongly suspect an error in lead placement — it is best to immediately repeat the ECG — after correct lead placement is verified. Sometimes, you may need to verify correct placement yourself. I know of no other way to ensure accurate interpretation of the ECG in question.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.