
Sent by Anonymous, written by Pendell Meyers
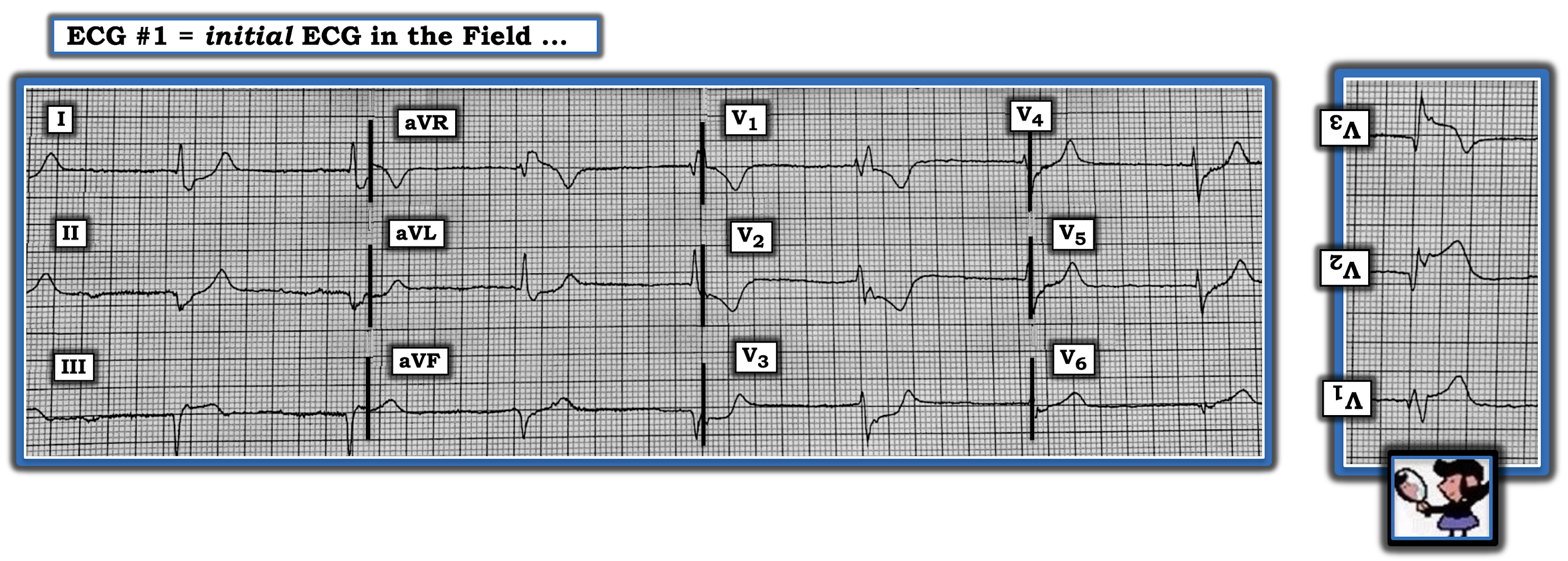
An elderly female called EMS for acute epigastric pain. EMS arrived and recorded this ECG on the way to the hospital:

This case was sent to me with only the details above, and my response was:
"It's posterolateral (and probably also inferior) OMI until proven otherwise. I'd also give a little calcium because it's slow, wide, and a couple leads have almost pointy Ts. But I don't really think it's hyperK. This one is OMI. Either LCX or RCA, or perhaps an Obtuse Marginal that supplies those regions."
Interpretation: There is an absence of sinus activity, including an absence of retrograde P waves. The rhythm is probably a junctional escape at a rate of approximately 45, with RBBB and likely also LAFB (given the leftward axis despite RBBB). Alternatively, it could be a posterior fascicular escape. There is STD in V2-V5 that is maximal in V2 and V3. This STD is excessively discordant in V2, and concordant in V3. The inferior leads show Q waves with STE in lead III, and there is some slight reciprocal STD in I and aVL. Interestingly, many of the T waves have a slightly peaked appearance. Along with bradycardia and conduction block, this would be alarming for potential hyperkalemia, which of course can also cause OMI mimics. We have shown several cases on this blog that appear to have both OMI and severe hyperkalemia.
Additionally, both 1) no spontaneous sinus activity (sinus arrest or extreme sinus brady) and 2) no retrograde activity, which implies AV block as well
Cardiology was summoned immediately to bedside but they thought that this ECG "isn't a STEMI" and refused to take the patient to the lab.
The initial troponin T returned highly elevated at 4.04 ng/mL. The potassium was 4.1 mEq/L. Cardiology was recalled to bedside to reevaluate.
Smith comment: When Pendell texted this to me, I thought it was both hyperkalemia and inferior posterior OMI. V4 and V5 especially have the appearance of hyperK. This just goes to show that there are always false positives and false negatives.
Another ECG was recorded:
 |
| These are almost certainly posterior leads, though they were not labelled as such (V4-V6 are really V7-V9 on the posterior thorax). How do we know? We can tell this because of the very low QRS amplitude and the Q-waves. The slight ST elevation is diagnostic of posterior STEMI, which in posterior leads only requires 0.5 mm in just one lead to meet "criteria." There are possible atrial waves but it is not definitive with this low quality ECG. If the possible atrial waves are real, it could be sinus bradycardia with 2:1 AV block. Otherwise, this would be complete heart block with junctional escape. The rate is approximately 30 bpm. Apparently the patient was mentating and had a normal blood pressure with this, and did not require pacing at that moment. |
The patient survived so far.
Learning Points:
RBBB should have a small, proportional amount of appropriately discordant STD and T wave inversion in leads with large R' wave (usually just V1 and V2). At some point, STD in these leads becomes out of proportion. This case is an excellent example of excessively discordant STD in RBBB, maximal in V2-V4, which signifies posterior OMI in RBBB.
Make sure to keep hyperkalemia on the differential for any sick patient with bradycardia, wide QRS, AV blocks, and bizarre morphology. It would have been an excellent choice to give this patient IV calcium on arrival to see if the ECG responded, while also treating for OMI simultaneously.

===================================
MY Comment by KEN GRAUER, MD (9/28/2020):
===================================
Superb interpretation of the presenting ECG in this case by Dr. Meyers!
- As per Dr. Meyers — the combination of QRS widening + bradycardia + lack of sinus P waves should immediately suggest the possibility of Hyperkalemia — especially since T waves in no less than 8/12 leads (ie, in leads I,II,aVL,aVF; and in V3-thru-V6) in the initial ECG look more-peaked-than-they-normally-should-be. For this reason — Dr. Meyers appropriately suggests that empiric Calcium would be a reasonable option in this circumstance, even before knowing the serum K+ level.
- NOTE — I would bet that No One who regularly follows Dr. Smith’s ECG Blog has trouble recognizing hyperkalemia when all of the typical findings are present. That said, many of our patients simply “don’t read the textbook” — and recognition of hyperkalemia becomes much more challenging when T wave peaking isn’t obvious (ie, when T waves aren’t so pointed with such a narrow base — or, when other abnormalities such as RBBB are present). For this reason — I thought it worthwhile to review some less appreciated ways in which hyperkalemia may present.
Regarding HyperKalemia & Brady Rhythms: We have previously discussed on numerous occasions in Dr. Smith’s ECG Blog, the multiple ECG manifestations of various degrees of HyperKalemia. Among these:
- Review of sequential ECG changes of Hyperkalemia — in My Comment at the bottom of the January 26, 2020 post.
- And, relevant to the bradycardia and lack of P waves in today’s tracing — My review of the mechanism for the various ECG changes (My Comment in the July 3, 2020 post) — which I restate here: The characteristic T wave peaking of hyperkalemia is seen early in the process — due to an acceleration by elevated K+ levels of terminal repolarization. With more severe K+ elevation — there is depression of conduction between adjacent cardiac cells, eventually with depression of SA and AV nodal conduction. This may result in a series of conduction defects, including PR and QRS interval prolongation — frontal plane axis shift — fascicular and/or bundle branch block (including interventricular conduction defects) — and/or AV block with escape beats and rhythms. Ultimately, QRS widening may lead to a sine-wave appearance (fusion of the widened QRS with the ST-T wave — such that distinction between the two is no longer possible). If this severe hyperkalemia remains untreated — VT, VFib or asystole are likely to result as the terminal event.
- As serum K+ increases — P wave amplitude decreases. Ultimately, P waves may disappear. This is because atrial myocytes are exquisitely sensitive to the extracellular effects of hyperkalemia (much more so than the SA node, AV node, the His, and ventricles). As a result — despite lack of atrial contraction (ie, loss of P waves on ECG) — there may still be transmission of the electrical signal from the SA node over the conduction system and to the ventricles. Thus, rather than a junctional rhythm or fascicular escape rhythm — a bradycardic rhythm without visible P waves in severe hyperkalemia may be a Sino-Ventricular Rhythm (in which despite lack of P waves on ECG — the rhythm IS still initiated in the SA node, with electrical transmission through to the ventricles). But because P waves disappear and the QRS is often wide with a hyperkalemic sino-ventricular rhythm — it is EASY to mistake this rhythm as either AIVR (Accelerated IdioVentricular Rhythm) or VT.
- BOTTOM Line: The bradycardia, altered P wave activity and the different forms of widened QRS morphologies may make for multiple potential ECG manifestations when there is severe hyperkalemia. The only way to prevent overlooking the diagnosis in some of these patients — is to always consider the possibility of HyperKalemia whenever presented with a tracing such as the one that was seen in today’s case.
— BUT — Serum K+ in this case turned out to be normal! Therefore — the ST-T wave appearance in today’s case is not the result of hyperkalemia.
QUESTION: If I were to show you the ECG that appears in Figure-1 — Would you have any doubt that this is an acute STEMI?
- HINT: The answer is “No”.

MY Thoughts on ECG #1: In the context of the obvious acute STEMI-like ST elevation in leads V1, V2 and V3 of Figure-1 — supportive ECG findings that we see in other leads should become unmistakably obvious:
- There is definite ST elevation in lead III — with reciprocal ST depression in high lateral leads I and aVL. These high lateral leads also manifest suspicious-looking terminal T wave positivity of surprisingly high amplitude.
- The T wave in lead II is obviously hyperacute (much more “voluminous” than-it-should-be, given modest depth of the S wave in this lead).
- In this context — the T wave in lead aVF is probably also hyperacute (given small depth of the S in this lead).
- All 3 of the lateral chest leads (leads V4,5,6) manifest clearly hyperacute T waves given modest QRS amplitude of the complexes in each of these leads. In addition, ST segments leading up to these hyperacute T waves are abnormal (depressed in V4; straightened in V5; and straightened with a rising takeoff in V6).
COMMENT: Despite the above described obvious abnormalities in 11/12 leads (actually in all 12 leads if you count the ST elevation in aVR) — in this elderly patient with new-onset potential chest pain “equivalent”symptoms — this case presents yet one more instance of the cardiology team stating, “Not a STEMI — therefore NO indication for acute cath.” I have to admit that I just do not understand this refusal ... (We’ve published many similar examples of this type of oversight — the most recent of which in our September 21, 2020 post).
CONFESSION: The 12-lead tracing I show above in Figure-1 was altered by me. I simply inverted the 3 leads within the RED rectangle (to project the mirror-image of leads V1, V2 and V3).
- I show the actual initial ECG in today's case in Figure-2 — to which I’ve added the inverted (mirror-image) view of leads V1, V2 and V3 to the right of ECG #1.
- As I’ve described in many prior posts on Dr. Smith's ECG Blog (See especially My Comment from Sept. 21, 2020) — the Mirror Test is no more than a simple visual aid that inverts anterior leads, thereby facilitating recognition of the shape of an acute posterior MI. It is based on the principle that the mirror-image of anterior leads provides insight into the appearance of ongoing electrical activity in the posterior wall. With a little practice — you’ll find posterior leads are rarely (if ever) needed — because use of the Mirror-Test allows instant recognition of virtually all cases when there is acute posterior MI.
- NOTE: Regardless of whether you call the ST-T wave appearance in the anterior leads of ECG #1 (in Figure-2) a “STEMI-equivalent” (since technically there isn’t ST “elevation” ) or simply an OMI — this pattern in a patient with new symptoms reliably identifies acute Occlusion-based MI.
- Final POINTS: The shape of the ST-T waves in leads V2 and V3 of ECG #1 in Figure-2 is clearly abnormal! Note how much J-point ST depression there is for the ST segment in lead V2. This is not seen with simple RBBB. The 2 mm of J-point ST depression with shelf-like straightening of the ST segment in lead V3 is also not a “normal accompaniment” of simple RBBB. Some ST-T wave depression is expected with uncomplicated RBBB — but generally this should be maximal in lead V1 (and not increasing as we move laterally toward leads V2, V3, as we see in Figure-2).

Thank you for great case again, and for this great blog. However, as an emergency physician I have one big question for Dr. Smith and co. You keep saying isolated ST-depression maximal (or purely isolated depression only) in V2-V4 should be considered as OMI and total occlusion, and saying posterior leads should NOT be taken.
ReplyDelete- However, "Of the 1,198 patients with isolated anterior (V1-V4) ST-segment depression, 314 (26.2%) had an occluded culprit artery (TFG 0/1)". Subjects with ST-elevation in any other leads (including posterior leads) were excluded. Thus 3/4 subjects with isolated anterior ST-depression had NOMI. I believe this is greatly contrary to your statement of isolated ST-depression in V2-V4 should be considered as OMI/STEMI-equivalent. https://doi.org/10.1016/j.jcin.2010.05.012
- In the following paper, it is stated that "23.5% had isolated ΔST elevation in ≥1 posterior lead without precordial ΔST depression." As such, the posterior leads should always be recorded since there can be ST elevation in V7-V9 without ST depression in leads V2-V4 https://doi.org/10.1016/S0002-9149(01)01431-X
- furthermore, in this paper "Posterior ST-elevation without ST-depression in V2-4 was present in 22% patients" https://doi.org/10.1016/S0735-1097(97)00538-X
- lastly, I believe you have only described one patient with ST-depression v2-4 with "falsely" negative posterior leads and acute OMI? http://hqmeded-ecg.blogspot.com/2013/01/precordial-st-depression-what-is.html
Any comment on these?
Thanks for your comment!
Delete-Regarding Pride et al, we are aware of this study and cite it in the OMI Manifesto etc. Many potential things to say about this. There are all kinds of reasons why we might not be talking about the same ECG patterns as Pride et al. are. When we talk about STD maximal in V2-V4, we always try to make sure we give the caveat that we exclude all patients with an abnormal QRS that could be causing appropriately discordant STD in V1-V4, for example RBBB should have a tiny bit of STD in V1-V2. So it is possible that, if Steve Smith were to identify a population with isolated STD in V1-V4, the rate of OMI would be higher than 26% they found. We have some data on STD maximal in V2-V4 coming out soon - we will certainly put out a blog post when this happens.
Second, their outcome is purely a TIMI flow grade 0/1, which is in my opinion too strict to catch all patients with real OMI. For example, Cox et al. (ref below) showed that 19% of obvious STEMIs had TIMI flow =3 of the lesion at the time of cath. So it is not surprising to me that only 26% of those patients in Pride et al. had TIMI 0-1. There is much more to the diagnosis of OMI than the TIMI flow snapshot at the time of cath. Finally, 26% is not an inconsequential rate of OMI even if that were the true number. All these NSTEMIs in Pride et al. need cath anyway, the only question is the timing - if you have a population that needs cath anyway, what percent of the population with OMI would warrant cathing them quickly vs. delayed? No one knows the answer to that.
(Am J Cardiol 2006.
Comparative early and late outcomes after primary percutaneous coronary intervention in ST‑segment elevation and non‑ST‑segment elevation acute myocardial infarction (from the CADILLAC trial). Am J Cardiol. 2006)
Regarding posterior leads: When you are not convinced about posterior OMI from the anterior leads, we recommend getting posterior leads because there is a portion of cases that are made easier to identify with posterior leads. When you ARE convinced about posterior OMI from the anterior leads, that is the scenario when we don't really see a good value of posterior leads. We have seen so many cases where posterior leads falsely reassured the provider and the clear posterior OMI was missed. You mention one case in which the posterior leads were truly negative, but we are also talking about situations like this case we are commenting on - even when the posterior leads BARELY show 0.5 mm (technically "positive"), people do not call them positive, instead in our experience people are somehow falsely reassured by how "small" and subtle the STE is in the posterior leads (due to low voltage). Indeed, in this very case above, the cardiologists did not believe that this posterior ECG met criteria.
Another similar case: https://hqmeded-ecg.blogspot.com/2020/04/guess-culprit-with-st-elevation-in.html
Another similar case: https://hqmeded-ecg.blogspot.com/2020/04/a-man-in-his-60s-with-chest-pain-st.html
Another: https://hqmeded-ecg.blogspot.com/2018/09/a-completely-healthy-30-something-woman.html
Another case where it is clearly positive but somehow the cardiologist doesn't agree because of the posterior leads: https://hqmeded-ecg.blogspot.com/2018/05/a-middle-aged-man-with-st-depression.html
In summary, we do not have a large amount of data confirming or denying our experience/claim that posterior leads can cause false reassurance. We recommend that posterior leads can be helpful when posterior OMI is a possibility but the anterior leads are not diagnostic. I stand by my personal claim that, in a patient with ACS, and a normal QRS that should not produce normal expected ST depression, then: STD maximal in V1-V4 is highly concerning to me for posterior OMI until proven otherwise. And I hope to publish on this soon! We finally have the database to answer this question.
First, I do not say not to record posterior leads. I say that if the initial 12-lead is diagnostic, do not record posterior leads. Better: record them, but understand their limitations.
DeleteHere are the problems with the Pride study:
There were too many important details missing from the methods:
1. Isolated ST depression that is maximal in right precordial leads V1-V4 is much more likely due to occlusion (usually circumflex) and reflect posterior STEMI
2. Isolated ST depression maximal in V4-V6 more often reflects subendocardial ischemia and an open artery.
Methods: For the present analysis, only patients with isolated anterior ST-segment depression in leads V1 to V4 were included. Patients with ST-segment elevation in other leads were excluded.
They excluded patients with ST Elevation, however:
1. Did they include patients who also had ST depression in left precordial leads V5 and V6?
2. Did they include patients who also had ST depression in limb leads?
Related:
3. Were patients included who had deeper ST depression in left precrodial leads V5 and V6 than in right leads V1-V4 included?
4. How many patients with MAXIMAL ST depression in V1-V4 were there, vs. MAXIMAL in V4-V6?
5. Was there any analysis comparing maximal in right vs. left precordial leads?
6. Were patients with < 1 mm of ST depression included?
7. Was there any subgroup analysis based on amount of ST depression?
Thank you for your explanations! I was not trying to be rude or anything, just wanted to hear your point of the view.
ReplyDeleteGood luck with your new papers, change can only be made with continuous (scientific) work. Love hearing from your studies and papers soon.
@ Unknown — You were NOT at all “rude”! I think it is great that you are asking the questions. As part of their ongoing research — Drs. Smith & Meyers have thoroughly reviewed the literature. Part of the problem as I perceive it — is too many in the cardiology community still negate the potential significance of OMI as an indication for prompt cath and reperfusion. “A picture is worth 1,000 words” — and among our goals on this ECG Blog is to show ACTUAL tracings that lack millimeter-definition of a stemi — yet which clearly suggest acute coronary occlusion. In the hope of constructive feedback — we call attention to cases in which the interventionist decision to cath was either delayed or refused — all with the goal of hoping to improve care in the future. Unfortunately, the cardiology literature still lags behind, and for the most part, has not yet caught up and acknowledged the concept of OMI. Please KEEP asking the questions!
Delete