
===================================
MY Comment by KEN GRAUER, MD (6/1/2020):
===================================
YOU are asked to interpret the ECG shown in Figure-1. Unfortunately, no history is available to assist.
- WHAT are the diagnostic possibilities for the rhythm?
- What are the prognostic implications of this rhythm?
 |
| Figure-1: The initial ECG in the ED. Please note that the long lead II rhythm strip is not simultaneously obtained with the 12-lead tracing above it. (See text). |
MY THOUGHTS on ECG #1: My initial impression on looking at the ECG in Figure-1 — was that the rhythm was either rapid AFib in a patient with WPW — or — PMVT (PolyMorphic VT). On looking closer — I realized that neither of these 2 possibilities was likely to be correct.
- QRS morphology varies in this tracing. Overall, the QRS complex looks wide — although in a number of leads, many of the beats look narrow. I suspect this is because part of the QRS complex in certain leads lies on the baseline. I thought the “theme” of this tracing was that the QRS is wide.
- I see no sign of atrial activity.
- The reason I initially thought the underlying rhythm was AFib — is that no atrial activity is seen in any lead and the rhythm “looks” irregular. However, on measuring R-R intervals with calipers — I was surprised to find that with rare exceptions (ie, beats #15, 16 and 17 in Figure-2) — the R-R interval remains constant for all other beats in the long lead II rhythm strip!
 |
| Figure-2: I have numbered the beats in the long lead II rhythm strip. As you look at this tracing — Keep in mind that this long lead II is not simultaneously obtained with the 12-lead tracing above it (See text). |
NEXT STEPS in Assessing ECG #1: The finding of precise regularity for the R-R interval for 25 of the 28 beats in the long lead II rhythm strip ruled out AFib as a possibility. This left me at this point with the following conclusions.
- The rhythm in ECG #1 was (except for 3 beats) — a regular WCT (Wide-Complex Tachycardia) rhythm.
- The ventricular rate was ~170/minute.
- QRS morphology varied in different parts of the tracing.
- There was no atrial activity.
Therefore — The diagnostic possibilities for the rhythm in Figure-2 would include: i) Some type of reentry SVT (SupraVentricular Tachycardia), in which QRS morphology was changing because of some unusual form of alternating aberrant conduction; or, ii) VT with a changing QRS morphology.
- Statistically — at least 80-90% of regular WCT rhythms without sign of atrial activity are VT. Given the QRS widening we see here, with bizarre, shifting QRS morphology (and improbability of so many supraventricular aberrant forms) — I thought the likelihood that this rhythm was some form of VT was at least 90-95%.
VT TERMINOLOGY: Before going further — it may help to review a number of terms that have been used to describe the morphologic appearance of various forms of VT. These include:
- Monomorphic VT — in which there is a similar (if not identical) QRS appearance throughout the episode of VT.
- Polymorphic VT (PMVT) — in which QRS morphology and/or axis continuously changes from one beat-to-the-next throughout the episode of VT. PMVT is not a regular rhythm — and it is often quite irregular. When PMVT is associated with a long QT interval — the rhythm is then defined as Torsades de Pointes (Please SEE My Comment at the bottom of the April 29, 2020 post in Dr. Smith’s ECG Blog).
- Pleomorphic VT — in which more than a single QRS morphology is seen during an episode of VT. Pleomorphic VT differs from PMVT — because QRS morphology is not changing from one beat-to-the-next. Instead, one QRS morphology will be seen for a number of beats — and then another morphology may take over and continue for another series of beats. Several different morphologies may be seen.
- Bidirectional VT — in which there is beat-to-beat alternation of the QRS axis. This unique and uncommon form of VT distinguishes itself from PMVT and pleomorphic VT — because a consistent pattern (alternating long-short cycles) is usually seen throughout the VT episode. As implied in its name, there are 2 QRS morphologies in bidirectional VT — and they alternate every-other-beat. (CLICK HERE — for a concise review + illustration of Bidirectional VT by Ali et al).
Let’s RETURN to Figure-2: Keeping the above 4 morphologic VT classifications in mind — WHICH ONE fits best for ECG-1?
MY Thoughts:
- The rhythm in ECG #1 is clearly not Monomorphic VT — because QRS morphology in Figure-2 is obviously changing throughout the long lead II rhythm strip.
- The rhythm is not Bidirectional VT — because the pattern of changing QRS morphology is not alternating every-other-beat. There is no consistent pattern to the changing QRS morphology in Figure-2.
- The rhythm in ECG #1 is also not PMVT — because the R-R interval is regular for almost all beats in this tracing — and, instead of QRS morphology changing from one-beat-to-the-next — there are several places in the tracing in which a similar QRS morphology seems to repeat itself for at least several beats in a row.
- Morphologically — I think the rhythm in the long lead II rhythm strip of ECG #1 is most consistent with a Pleomorphic VT.
COMPARE ECG #1 with ECG #2: I think the easiest way to make the case for Pleomorphic VT is to compare the 2 tracings in Figure-3:
- I took ECG #2 in Figure-2, from the October 12, 2013 post in Dr. Smith’s ECG Blog. The diagnosis of PMVT is readily apparent from the long lead II rhythm strip of ECG #2 — which shows a wide QRS complex, not resembling any known form of conduction block — in which QRS morphology continually changes from one-beat-to-the-next. Note also in the long lead II rhythm strip for ECG #2, how the QRS axis frequently shifts after every few beats — initially positive for a single beat — then negative — then positive in the middle of the tracing — then negative again — before turning positive for the last 7 beats in the tracing.
- Looking now at ECG #1 in Figure-2 — I found it interesting how in addition to manifesting a constant R-R interval for 25 out of 28 beats on the tracing — there was a limited number of QRS morphologies that tended to repeat. Keeping in mind that the long lead II rhythm strip at the bottom of ECG #1 is not simultaneous with the 12-lead above it — Note how the 8 QRS complexes in leads V1, V2, V3 look very much like monophasic VT. In the long lead II rhythm strip — Isn’t QRS morphology similar for beats #3,4,5; 7; 9; 11,12,13; 20,21,22; 24; 26; and 28? Doesn’t a 2nd QRS morphology tend to repeat itself for beats #1,2; 16; 18,19?
- Technically — the rhythm in ECG #1 does not satisfy the above textbook definition I gave for pleomorphic VT. But I think the uncanny R-R interval regularity (for 25 out of 28 beats in the long lead II) — and the unmistakable resemblance of so many beats to 2 different QRS morphologies places this rhythm closest to qualifying as Pleomorphic VT.
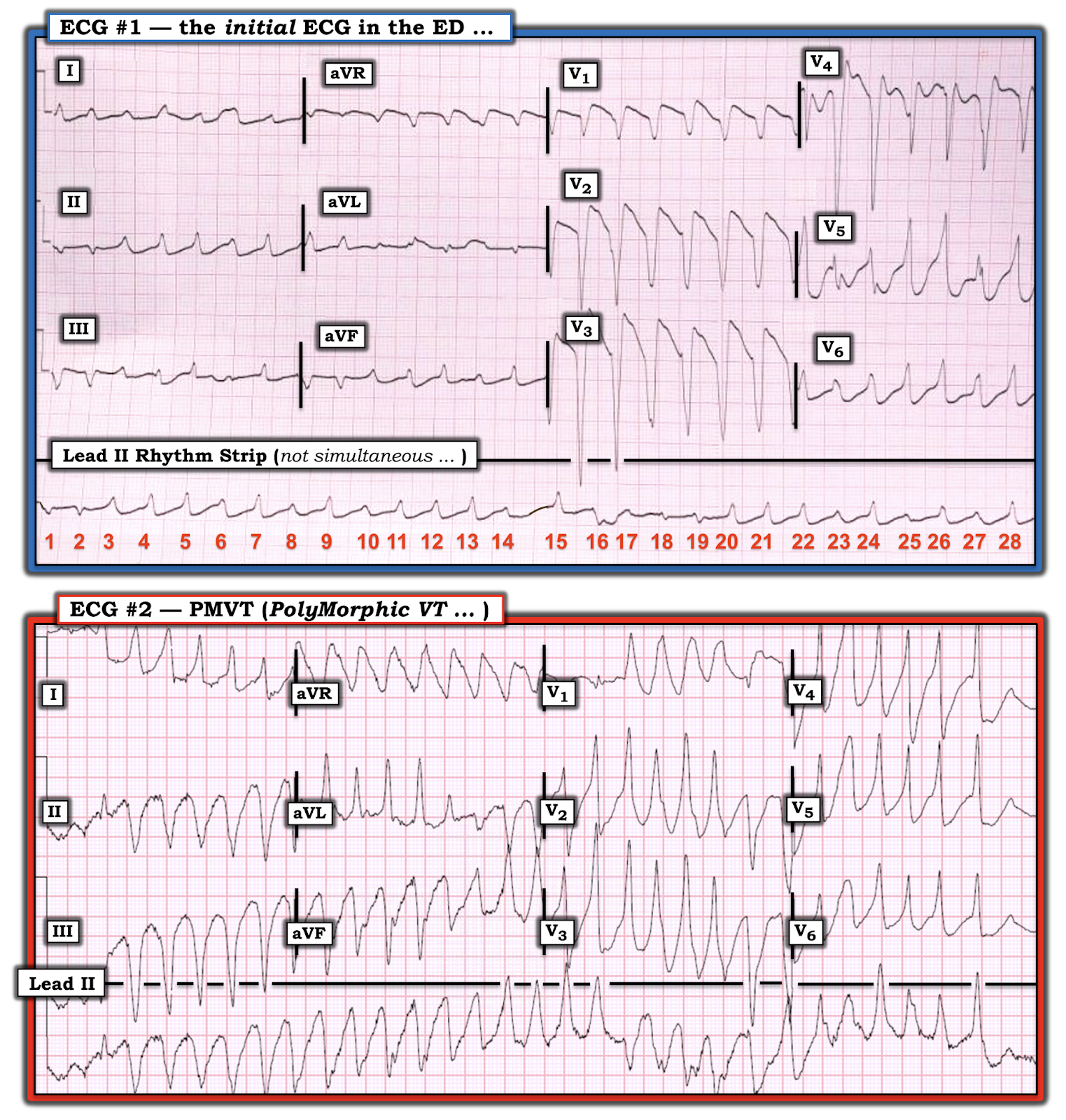 |
| Figure-3: Comparison of ECG #1 with an example of PMVT, that I took from the October 12, 2013 post from Dr. Smith’s ECG Blog (See text). |
WHY CARE about QRS Morphology with VT? Classification of the morphologic type of VT may provide clues to etiology, outcome and treatment.
- Monomorphic VT may occur in patients with or without underlying structural heart disease. Because the ventricular activation sequence is constant in monomorphic VT (which is why all beats look the same) — successful treatment (either by medication or cardioversion) is generally easier to accomplish.
- The occurrence of monomorphic VT in a patient without underlying structural heart disease (and without QT prolongation or metabolic/electrolyte abnormalities) — is known as Idiopathic VT. The “good news” — is that long-term prognosis of patients with idiopathic VT tends to be excellent.
- As noted earlier — Bidirectional VT is uncommon. Think of digitalis toxicity and catecholaminergic polymorphic VT as potential etiologies in which you are more likely to see bidirectional VT.
- PMVT is divided into 2 groups, depending on whether the preexisting QT interval is prolonged. The occurrence of PMVT in association with baseline QTc prolongation — is defined as Torsades de Pointes. Torsades often has a multifactorial etiology (ie, drug-induced, electrolyte depletion, CNS disturbance and/or other underlying disorder that may predispose to QT lengthening). KEY aspects of treatment include IV Mg++ (often at high dose) + finding and “fixing” the cause of the long QTc.
- In contrast — PMVT without QT lengthening most often has an ischemic etiology. Although IV Mg++ is also indicated as initial treatment of PMVT with a normal QT — it is clearly less likely to respond to IV Mg++, than when the QT interval is prolonged. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia.
- Pleomorphic VT is less well known than the other morphologic forms of VT. Patients with pleomorphic VT generally have significant underlying structural heart disease. A number of mechanisms have been proposed to explain the pattern of pleomorphic VT, in which there may be one or more runs of VT with a given similar QRS morphology — that is then punctuated by runs of VT with 1 or more other QRS morphologies. Potential mechanisms for explaining pleomorphic VT are complex — and include the possibility of: i) a single VT circuit with more than a single exit site; ii) the presence of more than a single VT circuit; and/or, iii) shifting conduction properties that alter the activation sequence (Liu & Josephson — Circ Arrhythm Electrophyiol 4:2-4 2011).
CLINICALLY — the important “take-home” point from this case, is that the shifting QRS morphology despite the constant ventricular rate we saw in ECG #1 — suggests the diagnosis of a pleomorphic VT. This entity appears to predispose to unstable reentrant conditions that increase the chance of deterioration from VT to PMVT or VFib.
- This may explain the poorer response of pleomorphic VT to antiarrhythmic therapy — and the higher morbidity and mortality that seems to be associated with this arrhythmia.
- Follow-Up to This Case: Although I did not learn specific details of this case — I did find out that this patient failed to respond to antiarrhythmic treatment and multiple shock attempts. He could not be resuscitated.
=====================
— My sincere appreciation to Zhang Mingming (of China) for contributing this case.
=====================
Ken...
ReplyDeleteWhat a great commentary on such a rare dysrhythmia! I have read (a little) about pleomorphic VTs but have never encountered one. And thank you for the very clear distinction between polymorphic and pleomorphic.
I was hoping you would comment on this case Jerry (!) — as it was also a learning experience for me. I didn’t find much in the literature … but was fascinated by this case that was sent to me. Every day = a learning experience! — :)
DeleteVTs that escalate from anatomically removed areas of heart can also initiate each other which can pleomorphism. Interesting that you compared polymorphic and pleomorphic in such detail.
ReplyDeleteThank you Steve! Polymorphic VT is the MUCH more common form of VT — so important to appreciate the specifics of what "pleomorphic" VT is — :)
DeleteGreat discussion of a fascinating tracing. I don't recall ever reading about pleomorphic VT (though maybe I've seen the word and my eye skimmed over it as "polymorphic"), and I've never seen a case in practice, but I've definitely seen the phenomenon a couple of times on various ECG forums and never had a name for it. Thank you so much for continuing to teach me new things after all these years Ken!
ReplyDeleteGreat to hear from you Vince! — :)
Delete