
A 50-something-year-old female with a history of an unknown
personality disorder and alcohol use disorder arrived via EMS following cardiac arrest with return
of spontaneous circulation. The described rhythm was an irregular, wide complex
rhythm. By EMS report, open pill bottles were found nearby at the scene, including quetiapine, fluoxetine, hydroxyzine, and gabapentin. She was successfully revived
after several rounds of ACLS including defibrillation and amiodarone.
On arrival to the ED the patient was intubated with normal vital
signs. An Initial ECG was performed:
Initial ECG:
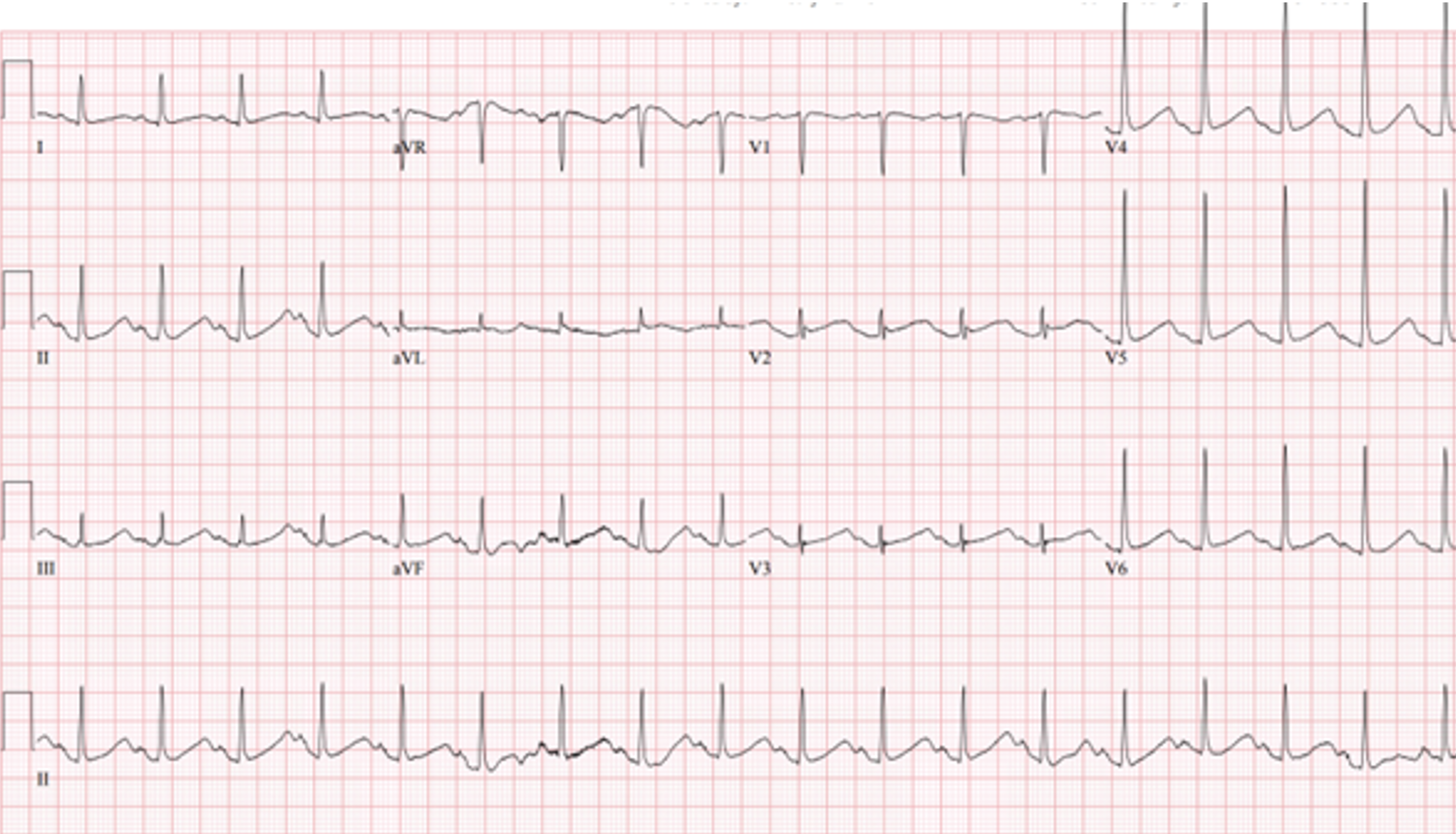 |
| Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). No ischemic ST changes. |
She was given magnesium empirically. Initial serum potassium level was 3.5 mEq/L, though the result was hemolyzed and was potentially lower than reported. Serum ionized calcium and magnesium levels were within normal limits.
A repeat ECG was performed 2 hours after arrival:
 |
| QTc prolongation at 722 ms now with alternating T wave pattern (T wave alternans) |

“T wave alternans and long QT. Portends Torsades de Pointes”
The patient was given additional magnesium and started on an
infusion of magnesium and a goal of high normal electrolyte repletion. She was
admitted to the ICU where subsequent ECGs were performed:
ECG at 12 hours
 |
| QTc prolongation, resolution of T wave alternans |
ECG at 24 hours
 |
| Sinus tachycardia with normalized QTc interval. |
She had an uneventful ICU course and was extubated for
ongoing care with the inpatient psychiatric service.
Teaching Points:
1. T wave alternans is characterized by variation
in T-wave morphology in the setting of consistent pacemaker and QRS morphology.
(1) TWA may be a result of heterogeneous in ventricular repolarization which
predisposes to polymorphic ventricular tachycardia (such as TdP). (2)
2. T wave alternans is a harbinger of cardiac
instability and TdP. (3)
3. QT prolonging medications and electrolyte derangement
are two common causes of QT prolongation and T wave alternans
References:
1.
Liu J, Hou H, Xu H, Chen Y,
Su X. Prolonged ST segment and T-wave alternans with torsade de pointes
secondary to hypocalcemia due to hypoparathyroidism: A case report. Ann
Noninvasive Electrocardiol. 2022 Jul;27(4):e12939. doi: 10.1111/anec.12939.
Epub 2022 Feb 11. PMID: 35146844; PMCID: PMC9296802.
2.
Molon G, Costa A, Bertolini L, Zenari L, Arcaro
G, Barbieri E, Targher G. Relationship between abnormal microvolt T-wave
alternans and poor glycemic control in type 2 diabetic patients. Pacing Clin
Electrophysiol. 2007 Oct;30(10):1267-72. doi: 10.1111/j.1540-8159.2007.00849.x.
PMID: 17897130.
3.
Narayan SM. T-wave alternans and the
susceptibility to ventricular arrhythmias. J Am Coll Cardiol. 2006 Jan
17;47(2):269-81. doi: 10.1016/j.jacc.2005.08.066. Epub 2006 Jan 4. PMID:
16412847.
4.
Moore PK, Raffel KE, Whitman IR. Macroscopic
T-Wave Alternans: A Red Flag for Code Blue. JAMA Intern Med. 2017 Oct
1;177(10):1520-1522. doi: 10.1001/jamainternmed.2017.3191.
5.
van Opstal JM, Schoenmakers M, Verduyn SC, de
Groot SH, Leunissen JD, van Der Hulst FF, Molenschot MM, Wellens HJ, Vos MA.
Chronic amiodarone evokes no torsade de pointes arrhythmias despite QT
lengthening in an animal model of acquired long-QT syndrome. Circulation. 2001
Nov 27;104(22):2722-7. doi: 10.1161/hc4701.099579. PMID: 11723026.
MY Comment, by KEN GRAUER, MD (10/23/2023):
- Clinically — electrical alternans is most commonly encountered in emergency medicine in association with supraventricular tachycardias (especially in the reentry SVT rhythms of AVRT and AVNRT).
- Electrical alternans is most commonly "looked for" — when considering pericardial effusion (although the "swinging heart" phenomenon that produces this ECG sign with this condition is rarely seen with smaller effusions).
- Today's post by Drs. Doyle, Palmieri and Bracey is especially noteworthy — because it presents the BEST example I have seen of T Wave Alternans.
- Electrical alternans is a general term that encompasses a number of different pathophysiologic mechanisms. Its occurrence is not limited to pericardial tamponade — but instead has been associated with an expanding array of clinical conditions.
- Distinction should be made between electrical and mechanical alternans. The term "alternans" itself — merely indicates that there is a phasic fluctuation in some cardiac signal from one beat to the next within the cardiac cycle. This may be in the strength of the pulse (or the blood pressure recorded) — or it may be in one or more waveforms in the ECG recording.
- Pulsus alternans — is a mechanical form of alternans. The rhythm is regular — but cardiac output varies from beat-to-beat. It is seen with severe systolic dysfunction. Pulsus alternans should be distinguished from a bigeminal pulse — in which a weaker beat follows the stronger beat by a shorter time interval (as occurs when the alternating beat is a PVC, which understandably generates less cardiac output).
- Pulsus alternans should also be distinguished from pulsus paradoxus — in which there is a palpable decrease in pulse amplitude (or a measured drop of >10 mm in blood pressure) during quiet inspiration. While pulsus alternans and paradoxus may both be seen with pericardial tamponade — they are different phenomena than the various types of electrical alternans.
- Electrical alternans — was first observed in the laboratory by Herring in 1909. It was reported clinically by Sir Thomas Lewis a year later, who characterized the phenomena as occurring, “either when the heart muscle is normal but the heart rate is very fast or when there is serious heart disease and the rate is normal”. This 1910 description by Lewis serves well to this day to remind us of the 2 principal clinical situations in which electrical alternans is most often encountered: i) Supraventricular reentry tachycardias; and, ii) Pericaradial tamponade.
- Repolarization Alternans — entails beat-to-beat variation in the ST segment and/or T wave. Alternation in ST segment appearance (or in the amount of ST elevation or depression) — is often linked to ischemia. In contrast — T wave alternation (which is what we see in Today's Case!) — is more often associated with changes in heart rate or in QT duration (especially when the QT is prolonged). In patients with a long QT — T wave alternans may forebode impending Torsades de Pointes.
- Both ST segment and T wave alternans have been known to precede malignant ventricular arrhythmias. Thus, this type of electrical alternans may convey important adverse prognostic implications when seen in certain situations.
- The above said — a variety of clinical conditions have been associated with repolarization alternans, such that adverse prognostic implications do not always follow. Among these clinical conditions are congenital long QT syndrome — severe electrolyte disturbance (hypocalcemia; hypokalemia; hypomagnesemia) — alcoholic or hypertrophic cardiomyopathy — acute pulmonary embolus — subarachnoid hemorrhage — cardiac arrest and the post-resuscitation period — and various forms of ischemia (spontaneous or induced by treadmill testing or other stimulus).
- Conduction and Refractoriness Alternans — entails variance of impulse propagation along some part of the conduction system. This may result from fluctuations in heart rate or in nervous system activity or from pharmacologic treatment. ECG manifestations from this form of alternans may include alternating appearance of the P wave, QRS complex or alternating difference in P-R or R-R interval duration. In particular — QRS alternans during narrow SVT rhythms has been associated with reentry tachycardias.
- NOTE: While identification of QRS alternans during a regular SVT often indicates retrograde conduction over an AP (Accessory Pathway) — this phenomenon has also been seen in patients with simple PSVT/AVNRT that exclusively limits its reentry pathway to the AV Node. Therefore — identification of QRS alternans during a regular SVT does not prove the existence of an accessory pathway. Conduction and refractoriness alternans may be seen with WPW-related as well as AV Nodal-dependent reentry tachycardias — atrial fibrillation — acute pulmonary embolus — myocardial contusion — and severe LV dysfunction.
- NOTE: On occasion — Alternans may be seen with monomorphic VT (Maury and Metzger).
- Cardiac Motion Alternans — is the result of cardiac movement rather than electrical alternation. The most important clinical entity associated with motion alternans is large pericardial effusion — though motion alternans has also been observed in some cases of hypertrophic cardiomyopathy. It is important to appreciate that not all pericardial effusions produce electrical alternans. That said — development of total electrical alternans (of P wave, QRS complex and T wave) — is likely to be a harbinger of impending tamponade.
- Unfortunately — the sensitivity of total electrical alternans is poor for predicting tamponade (ie, most patients who develop tamponade do not manifest preceding electrical alternans). Therefore, while it may be helpful if you do see total electrical alternans in a patient with a large pericardial effusion — Failure to see electrical alternans in no way rules out the possibility that tamponade is about to occur. Echo studies in patients with documented cardiac tamponade confirm that electrical alternans is synchronous with and a direct result of the pendulous movement of the heart within the enlarged, fluid-filled pericardial sac of a patient with large pericardial effusion (the "swinging heart" phenomenon).
- In practice — It appears that electrical alternans is most often seen in association with regular SVT rhythms (See the example in My Comment at the bottom of the page, in the September 7, 2020 post in Dr. Smith's ECG Blog). Seeing it in this context suggests (but does not prove) the existence of an AP (Accessory Pathway). Regardless of whether the mechanism of the regular SVT is AVNRT or AVRT — it is likely that reentry is involved. This conclusion may prove useful in contemplating potential investigative and therapeutic interventions.
- In a patient with pericarditis — OR — a large heart on chest X-ray — OR — simply unexplained dyspnea (as in the November 28, 2022 post) — recognition of electrical alternans should suggest the possibility of a significant pericardial effusion that may be associated with tamponade.
- Today's case of T Wave Alternans by Drs. Doyle, Palmieri and Bracey, is especially relevant clinically — because it alerts providers of a significantly increased risk of Torsades de Pointes if prompt correction of electrolyte disorders, as well as supplemental Magnesium is not promptly initiated.
- Finally — Although electrical alternans is a nonspecific ECG sign — recognition of this phenomenon may alert the clinician to look for myocardial ischemia, LV dysfunction and/or some other potential precipitating factor(s) that may have escaped initial assessment. BOTTOM Line: If you see electrical alternans — Look for an underlying clinical condition that may be responsible for this ECG sign.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.