
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer
A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chest pain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
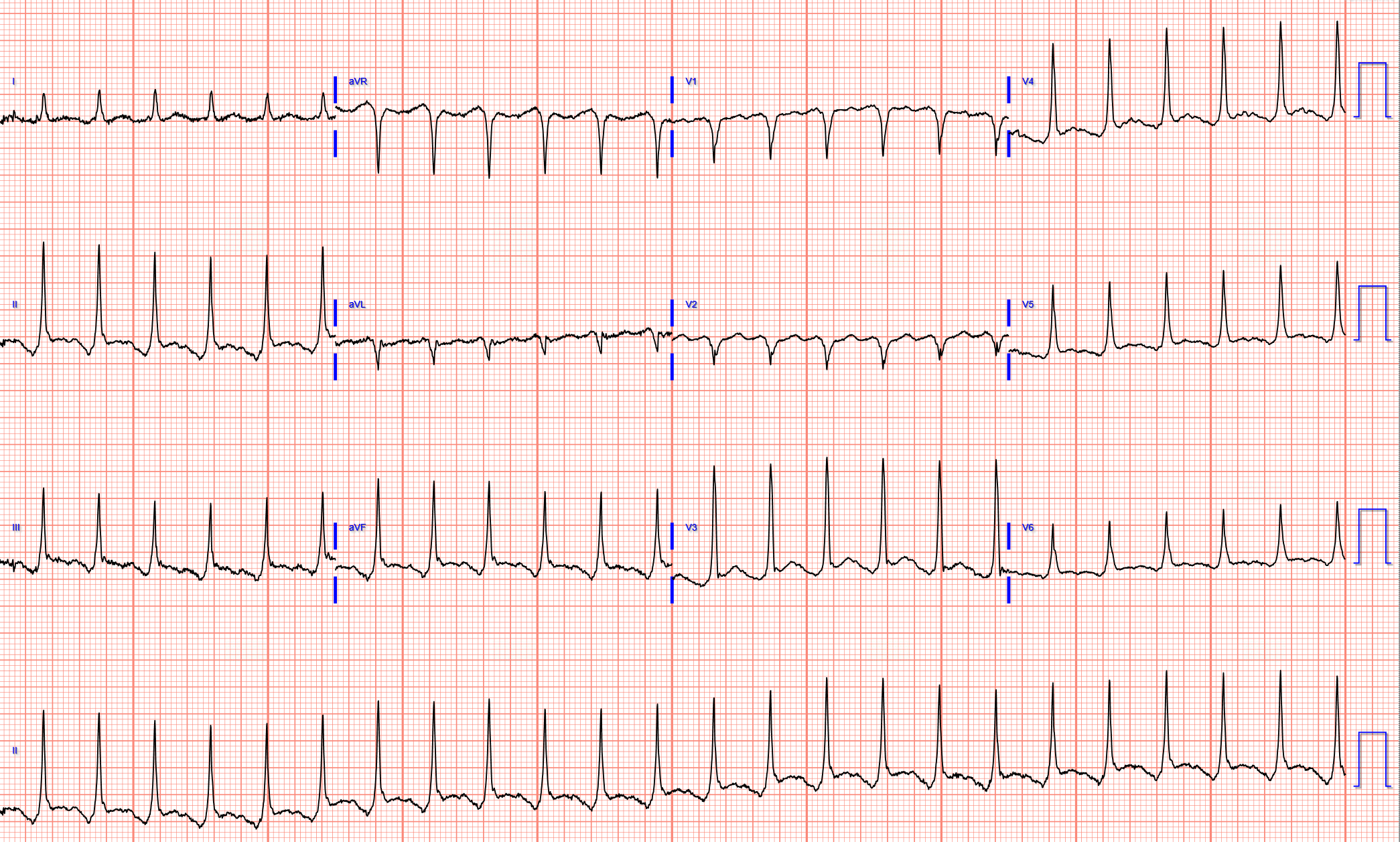
Triage ECG:
 |
| What do you think? |
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. In the limb leads, where we can see the ectopic atrial rhythm in this ECG, we see the classic situation of ectopic atrial P waves causing the illusion of inferior ST elevation which is more likely due to exaggeration of atrial repolarization ("Ta waves"). This situation has been named "Emery phenomenon."
In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way. It is a known OMI mimic that we have shown on the blog many times.
See these similar cases:
Here is the Queen of Hearts interpretation of the ECG above:

The patient had a baseline available for comparison:


The patient went back and forth into the abnormal rhythm during the initial ED course, and here is a full 12-lead of the abnormal rhythm:
 |
| It appears this one has barely managed to trick QOH. That is likely because she has not had many of these Emery phenomenon in her training yet. |
Unfortunately, this fooled the Emergency Physician and Cardiologist into an emergent angiogram for perceived "inferior STEMI."
The angiogram showed completely normal coronary arteries.
They rhythm returned to sinus reportedly after metoprolol IV was given.
The emergent echocardiogram showed normal EF, no WMA, and normal valve function.
Three serial high sensitivity troponins were below the limit of detection.
Next day ECG:
 |
| Normal variant STE, which of course casually meets STEMI criteria in some combination of leads V3-V6 at baseline, like many normal patients do. |

YOU TOO CAN HAVE THE PM Cardio AI BOT!! (THE PM CARDIO OMI AI APP)
If you want this bot to help you make the early diagnosis of OMI and save your patient and his/her myocardium, you can sign up to get an early beta version of the bot here. It is not yet available, but this is your way to get on the list.
Electrolytes and TSH were normal.
No use of drugs, stimulants, etc. was discovered.
Unfortunately the patient was erroneously diagnosed with "SVT / atrial fibrillation" and put on apixaban!!!
Hopefully his outpatient EP appointment will understand and correct that.
See more posts on the atrial repolarization wave:
K. Wang Video lecture: the Atrial Repolarization Wave (Ta Wave)
Look at this ST Depression
Atrial Repolarization Wave Mimicking ST Depression
![]()
===================================
MY Comment, by KEN GRAUER, MD (9/28/2023):
===================================
If I had to choose a title for today's case — it would be, "A Tale of 2 Findings". I found this fascinating case by Dr. Meyers unique in telling 2 storie lines:
- Story Line #1: Why is the inferior lead and chest lead ST elevation that is so evident on the initial ECG — not indicative of an acute STEMI?
- Story Line #2: What is the fast rhythm that kept occurring until the patient was treated with IV metoprolol?
For clarity in Figure-1 — I've adapted my figure in the February 23, 2023 post of Dr. Smith's ECG Blog, in which I illustrated the Emery Phenomenon that Dr. Meyers alludes to in his excellent discussion.
-USE.png) |
| Figure-1: Illustration of the Emery Phenomenon (adapted from My Comment in the February 23, 2023 post in Dr. Smith's ECG Blog — and — from the 2015 post by Dr. Bojana Uzelac on Armel Carmona’s ECG Rhythms website). The 2 sets of limb leads shown are from this Feb. 23, 2023 post — in which there is inferior lead ST elevation with the low atrial rhythm (to the LEFT) — with resolution of ST elevation after sinus rhythm was restored (to the RIGHT). = = = = = = = NOTE: The reason for the different sequencing of the limb leads in this Figure (which use a -aVR lead, that is sandwiched between leads I and II) — is that these 2 tracings were recording using the Cabrera Format (which I review in My Comment at the bottom of the page in the April 24, 2022 post). |
=====================================
What Happens with the Emery Phenomenon?
The top 2 schematic illustrations in Figure-1 — explain the theory involved in the Emery Phenomenon.
- An atrial repolarization wave (ie, the T of the P wave) is always present on ECG. With sinus rhythm, the timing of the Tp will largely coincide with the timing of the QRS complex — and therefore not be noticed on the ECG (dotted RED half circle, seen in the upper RIGHT schematic illustration in Figure-1).
- Note that the Tp is oppositely directed to the P wave. Therefore, with normal sinus rhythm (in which by definition, the P wave will be upright in lead II) — the TP will be negative, and be contained within the QRS complex.
- BUT — IF the P wave in lead II is negative (as may occur with either a low atrial or junctional rhythm) — then the Tp will be upright (dotted RED half circle, seen in the upper LEFT schematic in Figure-1). If the Tp wave is large in size and upright — it may distort the end of the QRS complex. And IF the PR interval of a large, negative P wave is short (ie, shorter than is shown in the upper LEFT schematic illustration) — then the upright Tp will be displaced to the right, producing the false impression of "ST elevation".
These effects of a large, negative P wave with a short PR interval on the subsequent ST segment — are seen in ECG #1 of Figure-1 (adapted from the February 23, 2023 post).
- The angled BLUE lines to the LEFT in Figure-1 — show ST segment straightening, and what looks to be significant ST elevation in the inferior leads of ECG #1.
- Later on in this Feb. 23, 2023 case — sinus rhythm resumes (RED arrow in the RIGHT figure, highlighting the upright P wave in lead II — with near resolution of the ST segment straightening and inferior lead ST elevation that had been seen in the LEFT figure).
=====================================
Application of the Emery Phenomenon to Today's CASE:
For clarity in Figure-2 — I've reproduced and labeled the initial ECG in today's case by Dr. Meyers. Note that I also added to this the long lead II rhythm strip done a little later in today's case, when the tachyarrhythmia recurred.
- The "beauty" of ECG #1 from today's case — is that it captures 7 beats of tachycardia with negative P waves in each of the inferior leads (YELLOW arrows) — after which sinus rhythm resumes, with upright P waves beginning with beat #8 in the long lead II rhythm strip (RED arrow over the upright P wave in front of beat #8).
- Note that the negative P waves in each of the inferior leads during the first 7 beats — manifest a fairly large negative deflection with a very short PR interval.
- Note especially that what appears to be "ST elevation" in each of the inferior leads during these first 7 beats — abruptly resolves the moment sinus rhythm resumes (seen wonderfully here by following the ST segment in the long lead II rhythm strip of ECG #1). This is the Emery Phenomenon. There was no true ST elevation in the inferior leads — only "pseudo-ST elevation" produced by the large upright Tp during the first 7 beats in which inferior leads had a large negative P wave with short PR interval!
- Finally — Note the very prominent J-point notching, with upward-sloping ST elevation in lead V4, that is virtually diagnostic of a benign repolarization variant.
-USE.png) |
| Figure-2: I've reproduced and labeled the initial ECG from today's case — to which I've added below the long lead II rhythm strip done a little later in today's case, when the tachyarrhythmia recurred. |
=====================================
What About the Tachycardia?
The question arises as to what is the recurrent tachycardia seen in today's case, up until treatment with IV metoprolol suppressed this rhythm?
- As always — I favor assessment of the 5 Parameters contained within the Ps, Qs, 3R Approach as the most user-friendly, time-efficient system for accurate rhythm interpretation (For more on the Ps,Qs,3Rs — See my January 26, 2023 post in Dr. Smith's ECG Blog).
Applying the Ps,Qs,3R Approach to the long lead II rhythm strip that appears at the bottom of ECG #1 in Figure-2:
- The first 7 beats seem to show a fairly Regular rhythm — with narrow QRS complexes — at a Rate of ~115/minute (R-R interval of ~2.6 large boxes in duration) — with negative P waves that are Related to neighboring QRS complexes with a short and constant PR interval.
PEARL #1: There is a differential diagnosis for the regular SVT (SupraVentricular Tachycardia) rhythm that we have just described — which in large part is based on the presence and nature of atrial activity (For more on distinguishing the various SVT rhythms — See My Comment at the bottom of the page in the March 6, 2020 post in Dr. Smith's ECG Blog).
- Today's regular SVT rhythm could be an ectopic atrial tachycardia (ATach) — or an automatic junctional tachycardia. (NOTE: Automatic junctional tachycardia is not common. ATach will be seen much more often in a nonselected practice. The fact that the PR interval of this negative P wave in lead II is short does not distinguish between these 2 entities. Initial emergency management is similar for both entities).
- Alternatively — Today's regular SVT rhythm could be the much less common "fast-slow" form of AVNRT (as I illustrate with laddergram in Figure-3 of My Comment in the March 6, 2020 post). And while initial treatment of all 3 of these SVT rhythms may be similiar (ie, The IV metoprolol that was successful in today's case will probably work for any of these SVTs) — the longterm management of ATach vs the "fast-slow" form of reentry SVT may differ.
PEARL #2: Did YOU notice HOW the 7-beat run of SVT in the long lead II rhythm strip of ECG #1 began? One of the most commonly overlooked Pearls of tachycardia interpretation — is the failure to look at HOW the tachycardia begins and ends. Admittedly — we often are not privileged to see this information. However, in ECG #1 — We see both the onset and offset of the SVT!
- The BLUE arrows that I drew in at the very beginning of leads II and III of ECG #1 — highlight that beat #1 in the long lead II rhythm strip is different! Because of where this ECG begins to record — we unfortunately do not see the QRS complex that occurs just before beat #1. But it is clear that the deflections under these BLUE arrows in leads II and III are different than the deflections under the 2 YELLOW arrows that follow. (QRS morphology of beat #1, especially in lead III — is also different than QRS morphology of beats #2-thru-7 that follow).
- The different QRS morphology of beat #1 is probably the result of aberrant conduction.
- The different deflection ( = T wave and/or T wave with PAC superimposed) under the 2 BLUE arrows to me suggested abrupt onset of today's SVT, most likely by a PAC. Initially this suggested to me that rather than ATach — the mechanism of today's SVT might be the fast-slow" form of AVNRT.
- BOTTOM Line: The above are advanced points that are academic because we cannot know what happened with beat #1 since we don't see the QRS before this beat. MY point that is relevant to optimal arrhythmia interpretation — is to always look to see if there is a "break" in the rhythm at the onset or offset of the tachycardia — since if present, this will often tell you the specific diagnosis!
PEARL #3: Ectopic ATach arises from an independent atrial focus. It is characterized by: i) P wave morphology different than morphology of sinus P waves (YELLOW vs RED arrows in ECG #1); ii) As opposed to the common reentry SVT rhythms (ie, "slow-fast" and "fast-slow" forms of AVNRT; and AVRT) that typically begin with one or more PACs — ATach often begins with a "warm-up" phenomenon (ie, gradual acceleration of the ectopic atrial focus) — and ATach often ends with a "cool-down" phenomenon (ie, gradual slowing of the ectopic atrial focus).
- Did YOU notice that the rate of today's SVT was significantly faster during the sustained SVT episode (ie, ~140/minute in the long lead II done later in the ED — compared to ~115/minute for the 7-beat run in ECG #1)?
- The fact that the rate of today's SVT was faster when the rhythm was sustained — but slowed down right before conversion to sinus rhythm (ie, with beat #8 in the long lead II of ECG #1) — suggests there was a "cool-down" phenomenon, as today's SVT gradually slowed until spontanenous conversion to sinus rhythm. This is much more consistent with ectopic ATach as the etiology of today's SVT.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.