
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers
Initial vitals: Temp 36.7 C, BP 161/79, RR 16, HR 70, Pulse Ox 97%
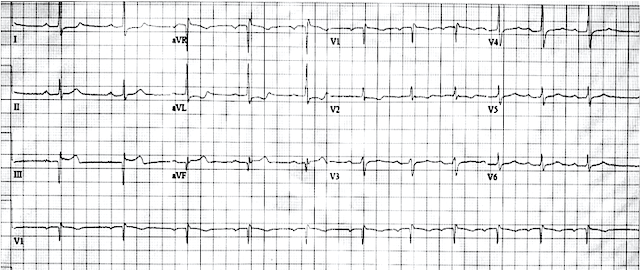
Initial ECG (during "minimal" pain):
 |
| What do you think? |
Meyers: I was sent this ECG with zero clinical information (and without the prior ECG below), and at that time I said that I did not see evidence of OMI. Yet there is minimal STE in III, some STD in I and aVL, and terminal T wave inversion in III, suggesting some reperfusion and consistent with the resolution of most of the pain. I should have seen that this could be inferior OMI with current reperfusion. If I had the history or the prior ECG below, I may have arrived at that diagnosis.
PM Cardio Queen of Hearts AI said "Not OMI - High Confidence". She is not able to compare to prior ECGs (yet).
Prior ECG on file:
 |
| Normal ECG, showing that the features above are new. |
He was treated initially with 325mg of ASA and 0.4mg SL NTG.
Bedside POCUS revealed inferior wall motion abnormality (images not available).
Smith comment: this is clearly an inferior OMI with reperfusion. Does it help to know there is a wall motion abnormality? Only if you are uncertain about the diagnosis of ACS. Reperfusion will usually NOT restore cardiac wall motion. The myocardium is "stunned" and will often (not always!!) remain hypo- or akinetic for some time even if not infarcted, just due to the profound ischemia incurred during the occlusive phase. Even many NOMI have wall motion abnormalities. Thus, an acute wall motion abnormality is not a sign of active or persistent ischemia, and thus is not necessarily an indication for emergent cath.
The EM physicians activated their "heart alert" pathway, which immediately summons the cardiology fellow to bedside to evaluate for potential emergent cardiac catheterization lab activation.
The interventional cardiologist was not initially convinced this was ACS and recommended CT pulmonary angiography to rule out pulmonary embolism.
The EM physicians activated their "heart alert" pathway, which immediately summons the cardiology fellow to bedside to evaluate for potential emergent cardiac catheterization lab activation.
The interventional cardiologist was not initially convinced this was ACS and recommended CT pulmonary angiography to rule out pulmonary embolism.
The pain returned/worsened, and the patient was then started on a nitroglycerin drip. Given the patients persistent and worsening pain and radiation to the back the team opted for a CT Aortogram.
High sensitivity troponin T, in ng/L:
After the 2nd troponin revealed a significant delta and given patients persistent pain a Heparin drip was started.
CT Aortogram revealed: No pulmonary embolism, No aortic dissection. "Decreased perfusion within the posterior descending artery territory suspicious for developing infarct."

Angiogram happened soon after:
LAD (mid): 80% stenosis
OM1 (prox): 80%
Ramus (ostial): 80% stenosis
RCA: 99% stenosis, no TIMI flow reported, felt to be culprit lesion, but for some technical reason unable to perform PCI and deemed more favorable for delayed CABG.
Here is the ECG with returning/worsening pain:
 |
| Increasing STE in III and aVF, increasing reciprocal STD in I and aVL. Inferior OMI until proven otherwise. OMI AI says "OMI - Low confidence" on this ECG. |
High sensitivity troponin T, in ng/L:
127 (12:00pm), 154 (1:05pm), 206 (2:25pm), none further measured.
Smith comment: an initial hs troponin (I or T) above 50 ng/L in a chest pain patient without a history of elevated troponin, cardiomyopathy, or end-stage renal disease has a very high positive predictive value for Acute MI (which in this case would be a type I MI), but does not differentiate between OMI and Non-OMI. (Large PE is also possible but this does NOT sound like a PE case). A delta is hardly necessary for the diagnosis and there is no delta which can differentiate OMI from NOMI. Therefore, a patient with persistent pain and a troponin at this level has Acute MI with ongoing ischemia and should go to the cath lab regardless of the ECG (this is by American and European guidelines).
After the 2nd troponin revealed a significant delta and given patients persistent pain a Heparin drip was started.
CT Aortogram revealed: No pulmonary embolism, No aortic dissection. "Decreased perfusion within the posterior descending artery territory suspicious for developing infarct."
Here is a screenshot of the image in question:

The arrow points to the area of ischemia. Subtle!
Angiogram happened soon after:
LAD (mid): 80% stenosis
OM1 (prox): 80%
Ramus (ostial): 80% stenosis
RCA: 99% stenosis, no TIMI flow reported, felt to be culprit lesion, but for some technical reason unable to perform PCI and deemed more favorable for delayed CABG.
I am not sure whether the patient had pain at the time of cath, but I suspect so.
Overnight the chest pain persisted, and ECG showed continued progression of OMI post cath (no intervention done):
Formal echo:
Hypokinesis of the inferior wall
EF 69% with globally normal systolic function
Normal LV thickness
No pericardial effusion
Clinical course:
1 day after admission: Intra-aortic balloon pump placed, exact indication uncertain
2 days after admission: 3 vessel CABG performed by Cardiothoracic Surgery: Venous grafting of OM and Ramus, LIMA to LAD, unable to intervene on RCA.
Overnight the chest pain persisted, and ECG showed continued progression of OMI post cath (no intervention done):

Formal echo:
Hypokinesis of the inferior wall
EF 69% with globally normal systolic function
Normal LV thickness
No pericardial effusion
Clinical course:
1 day after admission: Intra-aortic balloon pump placed, exact indication uncertain
2 days after admission: 3 vessel CABG performed by Cardiothoracic Surgery: Venous grafting of OM and Ramus, LIMA to LAD, unable to intervene on RCA.
The patient survived to discharge, but long-term follow up is unavailable.
No peak troponin was measured, and no TIMI flow was recorded, so it is not 100% definite that this case would meet the OMI definitions we have used in our studies so far. The culprit lesion with the ECGs above make me almost certain that this case meets the conceptual definition of OMI.
==================================
My Comment by KEN GRAUER, MD (4/9/2023):
==================================
The KEY point I'd like to emphasize regarding today's case is that a specific diagnosis of the "culprit" artery with acute OMI is less important than simple recognition that an acute cardiac event is ongoing.
- To illustrate this point — I've put the first 2 ECGs in today's case together in Figure-1.
My Initial Thoughts on Today's Case:
Like Dr. Meyers — I first saw ECG #1 without the benefit of any clinical history, other than knowing that this tracing was recorded in the ED.
- Most of the tracings we review from the ED are recorded in patients with some sort of chest pain history — though we were sent this tracing without knowing whether this CP (Chest Pain) was acute and ongoing — vs — present for several days and now resolved — vs — non-cardiac-sounding CP — vs — a "routine" ECG done for some other emergency disorder (ie, an acute abdomen) in a patient about to be taken to the OR.
- My Initial Reply regarding ECG #1: Is this ECG from a patient with CP? If so — I'm suspicious of recent infero-postero OMI. That said — I agreed completely with Dr. Meyers that ECG #1 was not specific for OMI.
- That said — as soon as I learned this patient's CP had significantly decreased (and was minimal) at the time ECG #1 was recorded — I felt my initial impression was supported, and that ECG #1 certainly could be consistent with recent OMI, now with reperfusion ST-T waves. Additional information would be needed for confirmation (ie, serial troponins — follow-up tracings, as well as search for a prior ECG) — but the onus was clearly on emergency providers to prove this tracing was not reflective of an acute ongoing event, rather than the other way around.
-USE.png) |
| Figure-1: Comparison of the first 2 ECGs in today's case. (To improve visualization — I've digitized the original ECG using PMcardio). |
What Does the Initial ECG Show?
The initial ECG in today's case clearly suggests that at some point in time — the patient has had an inferior infarction:
- The Q wave in lead III of ECG #1 is huge. There is also a significant Q wave in lead aVF — that is equal in depth to the height of the tiny R wave in this lead.
- As per Dr. Meyers — there is slight ST elevation in lead III, with terminal T wave inversion — as well as potential reciprocal changes (ST flattening and slight depression) in high-lateral leads I and aVL.
Subtle ST-T wave abnormalities are seen in virtually all of the remaining leads:
- There is nonspecific straightening of the ST segment in lead II.
- There is early transition — with abrupt appearance of a predominant R wave already by lead V2 (consistent with posterior MI at some point in time).
- Instead of gradually upsloping ST segments with upright T waves in leads V2-thru-V6 — T waves are barely seen, with nonspecific ST segment flattening in these leads (and with slight ST depression in lead V4).
BOTTOM Line for ECG #1:
- Prior inferior (and probably also posterior) infarction has occurred at some point in time.
- ECG #1 is not diagnostic of acute occlusion. That said, given the history in this 50ish year old man with risk factors, who describes 24 hours of worsening CP — with near resolution of CP at the time he finally arrived in the ED — ECG #1 is clearly consistent with a possible new infero-postero OMI, now with spontaneous reperfusion corresponding to the time the patient reports the decrease in CP (ie, In between the period of acute ST elevation and reperfusion T wave inversion — can be a phase of "pseudo-normalization", during which ST-T waves manifest diffuse flattening — but not much ST elevation or depression).
- Alternatively — ECG #1 might represent multi-vessel disease, on top of which there may (or may not be) ECG changes of another new event.
Benefit of the Prior Tracing:
Lead-by-lead comparison of ECG #1 with the prior ECG on file proved insightful:
- Q waves were previously present in leads III and aVF — albeit compared to R wave amplitude in these leads in the prior tracing — the Q waves in leads III and aVF of ECG #1 are now larger.
- ST-T wave appearance in each of the inferior leads is clearly different in these 2 tracings. A normal ST-T wave was previously seen in lead II. There was no ST elevation in lead III of the prior tracing, and the T wave was all negative instead of biphasic (up-down).
- ST-T waves looked normal in leads I and aVL of the prior tracing.
- In the chest leads — transition was not as abrupt (ie, a predominant R wave was not seen until lead V3 in ECG #2). There was no ST depression in lead V4 — and precordial lead T waves looked uniformly better in the prior tracing.
- IMPRESSION after the Prior Tracing was Found: There can no longer be any doubt that ST-T wave changes in ECG #1 are acute. Prompt cath was indicated at this point in the case.
Final POINTS:
- Even "after the fact" — I have trouble identifying the specific "culprit" artery from review of the initial ECG and the prior tracing on file — and, difficulty distinguishing the picture painted by these 2 ECGs from what might be seen with acute ischemia and multi-vessel disease. Clinically, this does not matter — since regardless, the patient's 24-hour history of CP in the context of obvious new ECG changes should merit prompt cath as soon as the prior ECG was found.
- P.S. — One wonders what took this patient with longstanding diabetes, hypertension and tobacco use a full 24 hours to make it to the ED. This patient is lucky he made it to the ED alive.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.