
Sent by Ali Khan MD, written by Pendell Meyers
A man in his 60s with HTN, HLD, known prior LBBB, presented with episodes of chest pain radiating to the left shoulder, with diaphoresis and dyspnea. Episodes started yesterday after starting to exercise, came and went throughout the day, and he decided to present to the ED the next morning after the one of these episodes failed to resolve like the others.
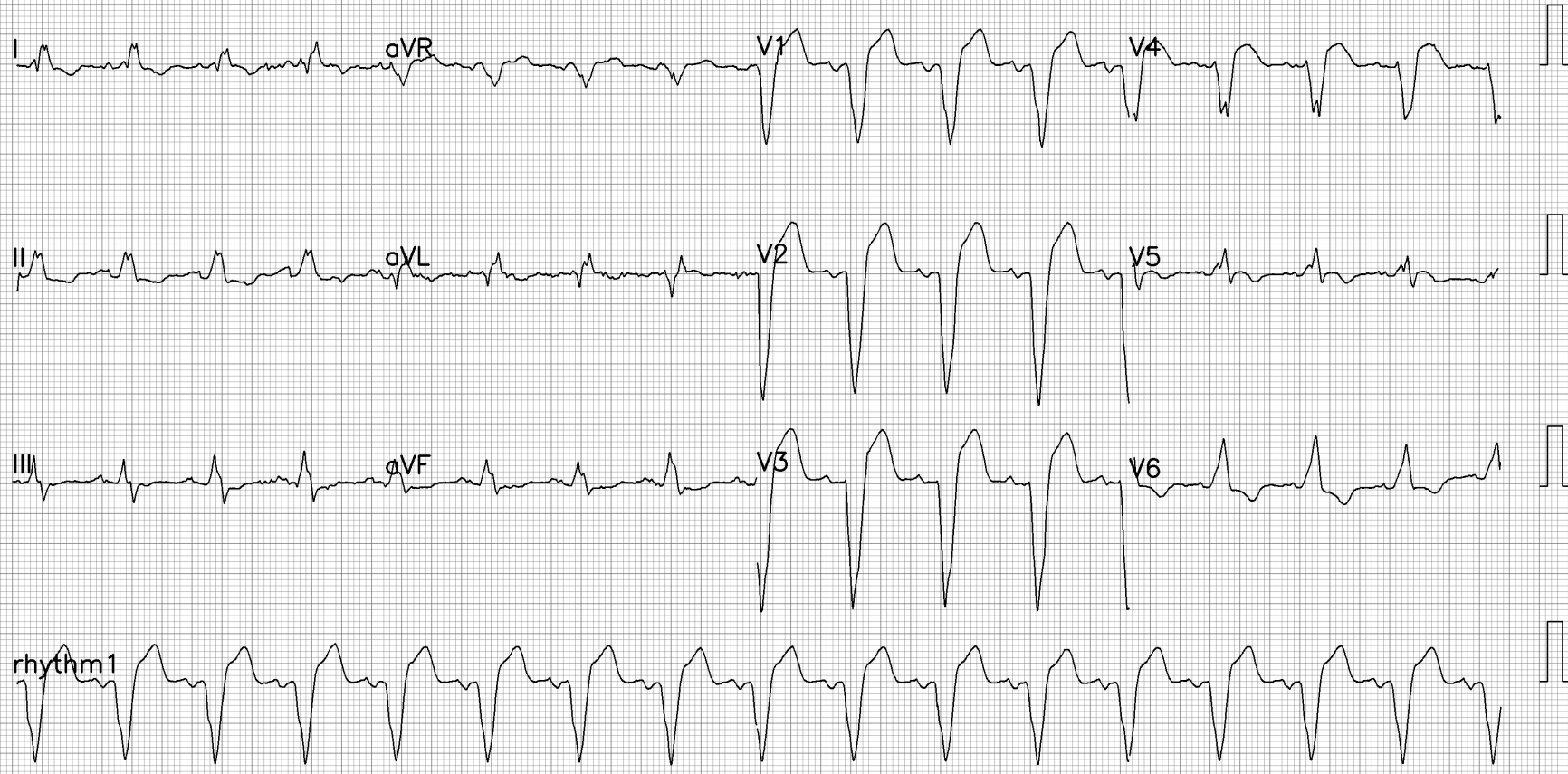
Here is his ECG at triage with ongoing pain (prior unavailable):

 |
| Same image optimized by PM Cardio app What do you think? |
I sent this to Drs. Smith, McLaren, and Grauer all of whom immediately diagnosed LAD occlusion based on modified Sgarbossa criteria (any concordant STE, any concordant STD in V1-V3 for posterior OMI in LBBB, or any excessively discordant STE). There is also concerning morphology in V1-V4 with likely hyperacute T waves and STT convexity.
Here are the STE/S measurements I make:
V1: 3.0 / 13 mm = 23%
V2: 4.5 / 15 = 30%
V3: 4.5 / 21 = 21%
V4: 3.0 / 9 = 33%
In our validation study of the modified Sgarbossa criteria, we chose the cutoff of 25% for excessive discordance to maintain high specificity (spec 99%, sens 80%). Using 20% resulted in 84% sens and 94% spec, meaning it was still quite specific. When there are multiple contiguous leads with even greater than 15%, the specificity is anecdotally still quite high. Additionally, this does not take into consideration comparison of ratios from baseline, which can be very helpful.
 | |
|
{kind=link}
Initial high sensitivity troponin came back at 6457 ng/L (no additional troponins drawn). Incidentally covid (+) with no respiratory or infectious symptoms.
 |
| Some reperfusion or evolution evident in V4, but V1-V3 still appear without significant reperfusion. I texted this to Dr. Smith and he texted back: "Incomplete reperfusion or lots of downstream platelet fibrin aggregates. Poor prognosis." |
As expected based on no reflow on ECG, the echocardiogram on day 2 showed:
Severely reduced LV systolic function. Severe global hypokinesis of the LV. EF 18%. Right ventricular function is normal.
No further follow up available.
Learning Points:
Use the modified Sgarbossa criteria to diagnose OMI in LBBB, ventricular paced rhythm, and generally all other significantly wide QRS complex morphologies.
The cutoff of 25% for excessive discordance was chosen with priority on specificity. 20% was still 94% specific, and we suspect that other situations are also specific (such as multiple contiguous leads with greater than 15%, increase ratio from known baseline).
Understand that the ECG is a better marker of reperfusion than the angiogram, unless one assessed myocardial perfusion grade, as graded by "blush".
Relationship of TIMI Myocardial Perfusion Grade to Mortality After Administration of Thrombolytic Drugs
OMI is not an ECG diagnosis, but often the ECG can make the diagnosis.
- The additional insightful feature from today's case by Dr. Meyers — is how skillful use of serial ECGs may at times provide a better indicator of successful reperfusion (or the lack thereof) than cardiac cath!
- CLICK HERE — For review article by Smith et al (with illustration on how measurements for assessing modified Smith-Sgarbossa criteria are obtained).
- Among the many cases of chest pain patients with LBBB that we have published in Dr. Smith's ECG Blog — the March 31, 2022 post by Dr. McLaren is especially insightful for illustrating how use of modified-Smith-Sgarbossa Criteria can facilitate rapid exclusion of acute OMI despite the presence of LBBB. (My Comment at the bottom of the page of this 3/31/2022 post then illustrates my use of qualitative criteria to assist in recognition of acute OMI with LBBB).
- To Emphasize: The ECG features that I describe below are not needed to diagnose acute OMI in today's initial tracing — because as discussed in detail by Dr. Meyers above, the finding of multiple contiguous leads with markedly elevated STE/S ratios in a patient with new chest pain is absolutely diagnostic. That said — I find it's always helpful to include assessment of all 12 leads in my decision-making — with the comforting reality that the more leads that show acute (or potentially acute) ST-T wave changes — the more solid is your diagnosis!
- What then do I mean by abnormal "qualitative" features? I look for ST-T wave changes that I know are not normal in a patient with LBBB. Some of these features are more specific than others — but taken together, the more abnormalities you see (in addition to your objective assessment for elevated STE/S ratios) — the more accurate I've found my interpretations to be.
-USE.png) |
| Figure-1: The initial ECG in today's case. (To improve visualization — I've digitized the original ECG using PMcardio). |
- The 4 chest leads cited by Dr. Meyers for clearly abnormal STE/S measurements ( = leads V1, V2, V3 and V4).
- Of these leads — I thought the shape of the disproportionately large, coved and elevated ST segment in lead V4 was definitely not consistent with "simple" LBBB.
- In this context — neighboring lead V5 (despite the small magnitude of its QRS complex) — showed clearly abnormal ST segment coving with unexpected T wave inversion. This is also not consistent with "simple" LBBB.
- Lead V6 is far more subtle — but in the context of neighboring leads V4 and V5 — the ST coving of this depressed segment is potentially a continuation of the coving seen in the prior leads. (To Emphasize — that by itself, I would not have interpreted the ST-T wave in lead V6 as abnormal!).
- High-lateral leads I and aVL both manifest a Q wave (which is not a normal finding with LBBB) — plus suggestion of ST segment coving that is, if not elevated — at least isoelectric (whereas the ST-T wave should normally be at least slightly depressed in these lateral leads with "simple" LBBB).
- Each of the inferior leads (II, III, aVF) — show abnormal ST flattening with slight ST depression. This is not usually seen with "simple" LBBB.
- To Emphasize: By itself — None of these ST-T wave changes in the limb leads are diagnostic. Instead — they are nonspecific findings that could be associated with ischemia, or which could be longstanding without any acuity. BUT — in association with clearly abnormal STE/S ratios in 4 chest leads — and the definitely abnormal morphologic ST-T wave findings in leads V4,V5 — I thought it a good bet that each of the 11 leads I highlight above were showing their version of acute changes.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.