
Written by Pendell Meyers
A man in his 60s presented with 1 hour of acute chest pain. Vitals were within normal limits.
Here is his triage ECG:
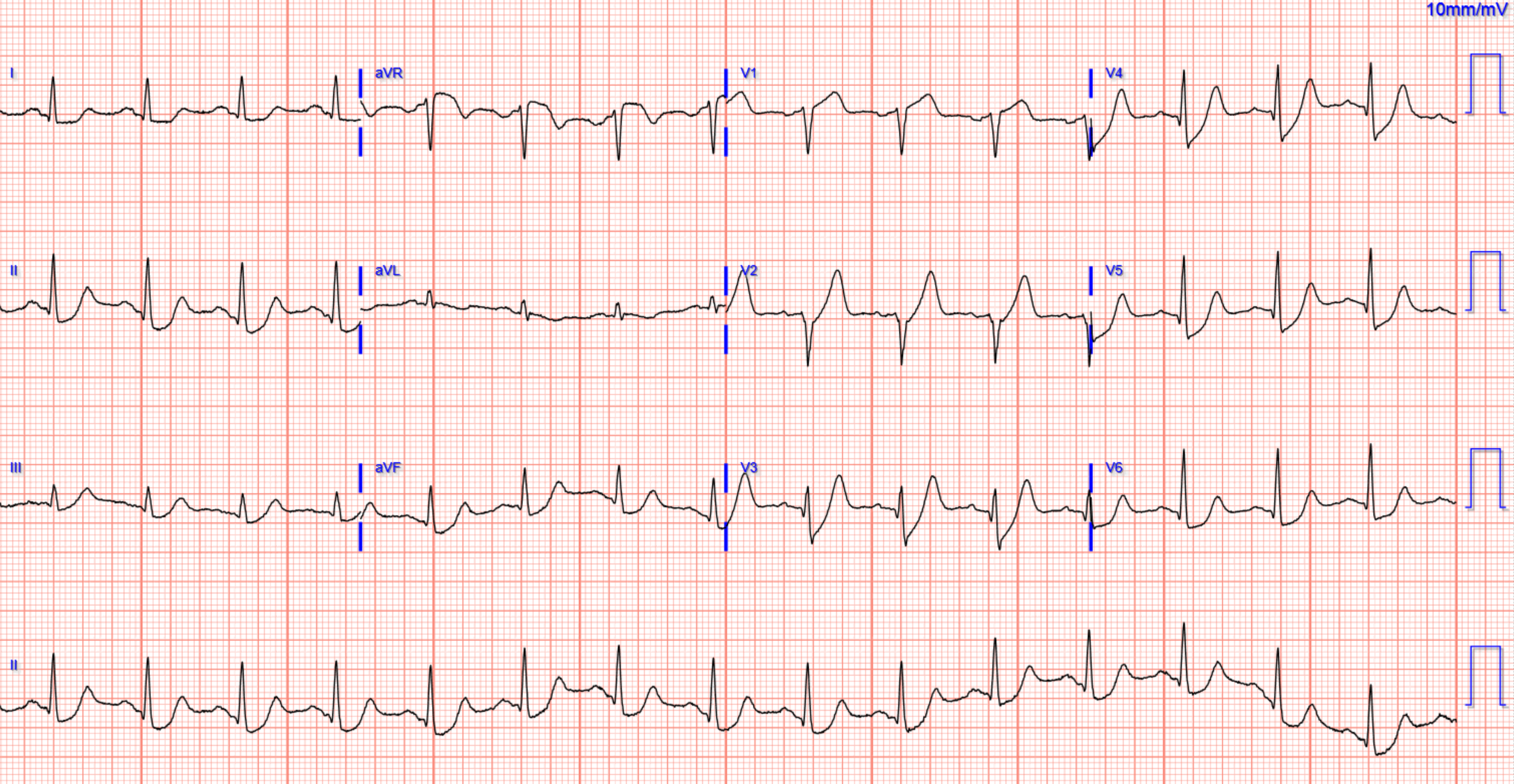

The ECG is a classic, pathognomonic ECG for acute LAD OMI. There is STE in V1 and de Winter morphology (hyperacute T wave with depressed ST takeoff / ST depression) in V2-V4. In the lateral leads V5-V6 and I and aVL there is STD that is likely in part reciprocal to the STE in V1. Also reciprocal STD in II and aVF, or potentially also de Winter morphology in inferior leads as well. With hyperacute T wave and STE in V1 and STD in V5-6, this constitutes an LAD OMI pattern that we are currently studying that we will be describing soon.
I do not think this ECG is possible in any other context other than acute cessation of blood flow to an anterior coronary artery. It is pathognomonic in my experience.
Of course, it has nothing even close to STEMI criteria.
The excellent provider understood the ECG immediately, and activated the cath lab. He persuaded the cardiologist to cath the patient emergently despite lack of STEMI criteria.
Cath: 100% (TIMI-0) thrombotic occlusion of the mid LAD, stented
First troponin returned at 441 ng/L.
All subsequent troponins were greater than 25,000 ng/L.
ECG immediately after cath:


Echo:
EF 45%
hypokinesis of mid-apical anteroseptal, anterior, inferoseptal, apical inferior, and apical myocardium
Learning Points:
You must understand and recognize hyperacute T waves and de Winter morphology if you want to provide excellent care for ACS patients.
===================================
MY Comment by KEN GRAUER, MD (7/11/2022):
===================================
- Because of the importance of this entity — we continue to periodically review it in cases we present (See the May 2, 2019 post — among many others).
De Winter T Waves:
In 2008 — Robert J. de Winter and colleagues (Drs. Verouden, Wellens, and Wilde) submitted a Letter to the Editor to the New England Journal of Medicine (N Engl J Med 359:2071-2073, 2008) — in which they described a “new ECG pattern” without ST elevation that signifies acute occlusion of the proximal LAD (Left Anterior Descending) coronary artery.
- The authors recognized this pattern in 30 of 1532 (~2%) patients with acute anterior MI. Cardiac cath confirmed LAD occlusion in all cases — with ~50% of patients having a "wraparound" LAD. Left mainstem occlusion was not present.
- This was the authors’ original description of the new ECG pattern: “Instead of the signature ST-segment elevation — the ST segment showed 1-3 mm of upsloping ST depression at the J point in leads V1-to-V6 — that continued into tall, positive symmetrical T waves”.
- The QRS complex was usually not widened (or no more than minimally widened).
- Most patients also manifested 1-2 mm of ST elevation in lead aVR.
 |
| Figure-1: The de Winter T Wave Pattern, as first described by Robbert J. de Winter et al in N Engl J Med 359:2071-2073, 2008. ECGs for the 8 patients shown here were obtained between 26 and 141 minutes after the onset of symptoms. (See text). |
In their original 2008 manuscript — de Winter et al went on to describe the following additional features:
- “Although tall, symmetrical T waves have been recognized as a transient early feature that changes into overt ST elevation in the precordial leads — in this group of patients, this new pattern was static, persisting from time of the 1st ECG until the pre-cath ECG.”
- Hyperkalemia was not a contributing factor to this ECG pattern (ie, Serum K+ levels on admission were normal for these patients).
NOTE: Technically speaking — the de Winter T wave pattern as described in 2008 by de Winter et al differs from the finding of simple "hyperacute" anterior T waves — because ECG findings with a strict de Winter T wave pattern persist for an hour or more until the “culprit” LAD vessel has been reperfused.
- As I note above (and as illustrated in the example ECGs taken from the de Winter manuscript that are shown in Figure-1) — there should be involvement in all 6 chest leads with the strict de Winter pattern, with most leads showing several mm of upsloping J-point ST depression and extremely large T waves.
MY Observations regarding De Winter T Waves:
Over the past decade — I have observed literally hundreds of cases in numerous international ECG-internet Forums of de Winter-like T waves in patients with new cardiac symptoms.
- Many (most) of these cases do not fit strict definition of “de Winter T waves” — in that fewer than all 6 chest leads may be involved — J-point ST depression is often minimal (if present at all) in many of the chest leads — and, the number of leads that manifest overly large T waves is limited.
- ECG changes in many of the cases that I have observed are not “static” until reperfusion (as had been initially reported in 2008 by de Winter et al.). Neveretheless, cath follow-up has routinely confirmed LAD occlusion in almost all cases.
- While many of these patients do not manifest “true" de Winter T waves” (because their ECG pattern does not remain static until reperfusion by coronary angioplasty) — for the practical purpose of promptly recognizing acute OMI — I do not feel ( = my opinion) it matters whether a “true” de Winter T wave pattern vs simple “hyperacute” T waves (that are de Winter-like) are present.
Regarding Today’s Case:
Despite my above disclaimer — the initial ECG in today’s case is remarkable for how closely it does follow the description (and illustration in Figure-1) of de Winter T waves from the original NEJM manuscript — which is why Dr. Meyers called this ECG "classic" and "pathognomonic" for acute LAD OMI.
For clarity — I've reproduced today’s initial tracing in Figure-2. Note the following:
- ST-T wave abnormalities are prominent in all 6 chest leads.
- There is significant J-point ST depression in 5 of the chest leads. This J-point ST depression begins in lead V2 — attains 3 mm in leads V3 and V4 — and continues through until lateral chest lead V6 (RED arrows in Figure-2).
- Arising from this J-point ST depression — is a rapidly rising (upsloping) ST segment that culminates in tall, positive symmetrical T waves (most marked in leads V2-thru-V4).
- The QRS complex is not widened.
- There is 1-2 mm of ST elevation in lead aVR.
- KEY Point: ECG #1 does not satisfy criteria for a “STEMI” — because there is not enough ST elevation. Regardless (as per Dr. Meyers) — it should still be immediately apparent in this patient with new-onset chest pain, that acute proximal LAD occlusion must be assumed until proven otherwise!
-USE.png) |
| Figure-2: I've labeled the initial ECG in today's case. |
- Small-but-significant Q waves are present in multiple leads in Figure-2 (BLUE arrows). Although the inferior lead q waves are extremely small and narrow — in view of the de Winter group's finding that ~50% of the patients in their study had a "wraparound" LAD — inferior (as well as anterior) infarction should be looked for.
- There is loss of r wave from lead V1-to-lead V2 (within the BLUE circle). Although the reduction in r wave amplitude between these 2 leads is tiny — we know it is "real" — because there is a definite Q wave in lead V3 (BLUE arrow in this lead). While the isolated finding of a small and narrow q wave (as seen in leads V5,V6) would not by itself be abnormal — extension of chest lead Q waves to as early a lead as V3 is clearly not "normal" (especially given "loss of r wave" from V1-to-V2). These abnormal chest lead Q waves provide clear indication of anterolateral infarction — and should be followed with serial tracings.
- I found the ST-T wave in lead V1 of Figure-2 interesting. The straight ST segment take-off and J-point elevation that we see is markedly abnormal for this initial chest lead — and would seemingly suggest a more proximal LAD site of occlusion.
- Reciprocal ST-T wave depression in each of the inferior leads in ECG #1 — also suggests a more proximal LAD site of occlusion.
- On the other hand — there is no ST elevation in either lead aVL or lead I (with lead I instead showing ST depression). Lead aVL especially — usually manifests at least some ST elevation when acute LAD OMI is proximal in location unless there is attenuation of ST elevation in lead aVL because of simultaneous inferior infarction from a "wraparound" LAD (which produces inferior ST elevation and reciprocal ST depression in aVL).
- That said — awareness of the above "additional" ECG findings that I have highlighted will be helpful in appreciating the course of evolution that this case will take (be it the result of a "wraparound" LAD OMI with simultaneous inferior infarction and/or associated multivessel disease).
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.