
A man in his 50s with a past medical history of hypertension and tobacco use disorder, who tested COVID positive 11 days prior, presented to the emergency department with worsening shortness of breath over several days. He was tachypneic and hypoxemic down to as low as 44% with reportedly good SpO2 waveform before EMS applied noninvasive ventilation with improvement to 85-89%. Although history was limited by extremis, the report is that there was no chest pain at initial presentation, only shortness of breath.
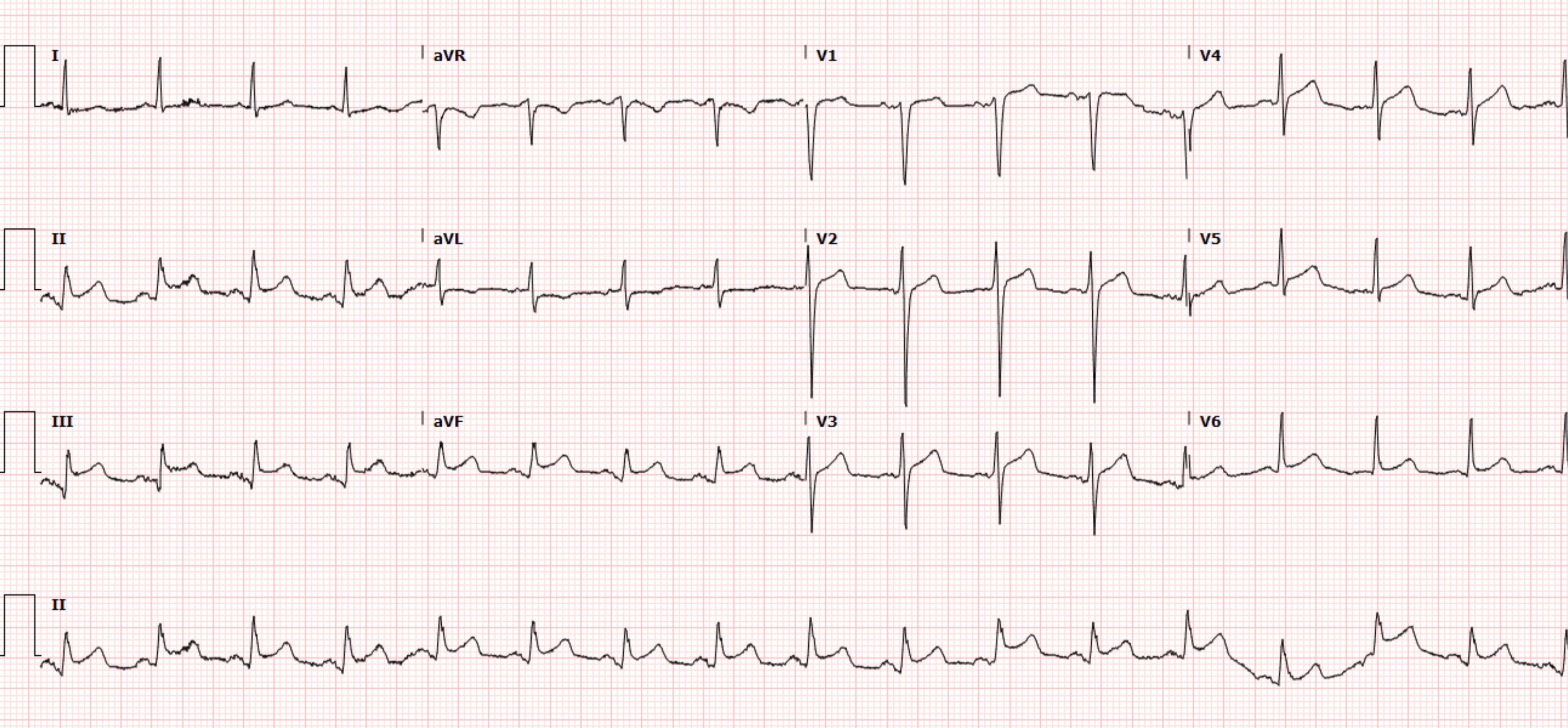
Here is his ECG on arrival, Day 1 around 0530:
 |
| What do you think? |
I see some small ST depression in V3-V6, II, III, aVF, and very small reciprocal STE in aVR. In the context of known covid with severe hypoxemia and respiratory distress, I would likely feel that this ECG most likely represents subendocardial ischemia, which is well explained by hypoxemia and respiratory distress.
Evaluation was remarkable for acute hypoxemic respiratory failure secondary to COVID-pneumonia and the patient was initiated on BiPAP and admitted to the ICU. It seems that no troponin was ordered so far. While boarding in the emergency department awaiting an ICU bed, the patient developed acute onset substernal and left sided chest pain, without any worsening of his shortness of breath or any escalation in his oxygenation/ventilation parameters or work of breathing. A repeat ECG was obtained:
ECG 2 - Day 1 around 1700:
Overall the QRS is unchanged, but there is new large STE in V1-V4, as well as tiny STE in II, III, and aVF. In comparison to the first ECG, we also see that the T waves are hyperacute in all the same leads. The slight STD in V6 is reciprocal to the right precordial STE, and the downsloping STD and TWI in aVL is reciprocal to the inferior STE/hyperacute T waves. This is diagnostic of anterior and inferior/apical OMI until proven otherwise. Pericarditis should not have any reciprocal STD or TWI. This is NOT DIFFUSE ST ELEVATION - this is focal. This suggests occlusion of a "wraparound" LAD do the inferior wall.
ECG 2 was interpreted by the Emergency Physician as sinus rhythm with ST elevations throughout inferior and precordial leads.
The ED physician activated a code STEMI and empirically treated for ACS - ASA, atorvastatin, and heparin gtt. Cardiology was called to the bedside. The cardiologist felt the ECG more likely represented myo-pericarditis in the setting of COVID19 rather than a Type I MI, and requested for a comprehensive echocardiogram to be obtained emergently. A limited stat bedside echocardiogram was performed and demonstrated anteroseptal and apical hypokinesis with a low-to-normal LVEF in the range of 45%.
The first troponin was ordered right after this ECG, which soon returned highly elevated at 3,555 ng/L.
Despite asking for the echocardiogram ostensibly for identifying wall motion abnormalities, the cardiologist still insisted that the patients overall clinical picture was more consistent with myo-pericarditis. He refused to take the patient to the cath lab. The patient went to the ICU with ongoing chest pain (now on high flow nasal cannula for oxygen requirement).
ECG 2 - Day 1 around 1700:
 |
| What do you think now? |
Overall the QRS is unchanged, but there is new large STE in V1-V4, as well as tiny STE in II, III, and aVF. In comparison to the first ECG, we also see that the T waves are hyperacute in all the same leads. The slight STD in V6 is reciprocal to the right precordial STE, and the downsloping STD and TWI in aVL is reciprocal to the inferior STE/hyperacute T waves. This is diagnostic of anterior and inferior/apical OMI until proven otherwise. Pericarditis should not have any reciprocal STD or TWI. This is NOT DIFFUSE ST ELEVATION - this is focal. This suggests occlusion of a "wraparound" LAD do the inferior wall.
ECG 2 was interpreted by the Emergency Physician as sinus rhythm with ST elevations throughout inferior and precordial leads.
The ED physician activated a code STEMI and empirically treated for ACS - ASA, atorvastatin, and heparin gtt. Cardiology was called to the bedside. The cardiologist felt the ECG more likely represented myo-pericarditis in the setting of COVID19 rather than a Type I MI, and requested for a comprehensive echocardiogram to be obtained emergently. A limited stat bedside echocardiogram was performed and demonstrated anteroseptal and apical hypokinesis with a low-to-normal LVEF in the range of 45%.
The first troponin was ordered right after this ECG, which soon returned highly elevated at 3,555 ng/L.
Despite asking for the echocardiogram ostensibly for identifying wall motion abnormalities, the cardiologist still insisted that the patients overall clinical picture was more consistent with myo-pericarditis. He refused to take the patient to the cath lab. The patient went to the ICU with ongoing chest pain (now on high flow nasal cannula for oxygen requirement).
There is no mention of anyone considering thrombolytics, all notes simply state that cardiology did not feel that the patient was having ACS. Yet they documented that cardiology recommended heparin drip, so that was given.
Serial ECGs and troponins were trended.
Serial ECGs and troponins were trended.
ECG 3 - Day 1 1750

ECG 4 - Day 1 1825

ECG 5 - Day 2 0000

Subsequent hs-troponins were 6,892 ng/L, then 9,110 ng/L, and then peaked at 10, 126 ng/L during this morning.
ECG 6 - Day 2 0921

The comprehensive echocardiogram resulted on Day 2 at 1048 and was remarkable for a reduced LVEF of 40%, proximal and mid anteroseptal hypokinesis, and distal anteroseptal and apical akinesis.
Cardiology still felt the patient’s presentation was more likely the result of myo-pericarditis.
ECG 7 - Day 3 1210
 |
| Anterolateral reperfusion without inferior reperfusion This sometimes happens when an LAD thrombus in a wraparound LAD embolizes to the apex, resulting in anterior reperfusion but persistent inferior occlusion. |
ECG 7 demonstrated evidence of coronary reperfusion with T wave inversions in the precordial leads - consistent with the OMI reperfusion sequence. This ECG further proves that the patient’s chest pain was the result of ACS rather than myo-pericarditis.
Day 4:
 |
| Anterolateral reperfusion, but active OMI in inferior leads likely corresponding to the apex, or less likely inferior septum. |
 |
| Mostly the same as prior, except that the anterior leads are not proceeding down the reperfusion progression (which would show enlarging TWI), instead they appear to be turning around and going the other direction: reocclusion? Look at V3. It is trying to transition from reperfusion to reocclusion findings. |
Without reasoning documented, troponins start getting ordered again around this time.
hs Troponin I:
2,008 ng/L
3,831 ng/L
 |
| Full re-ooclusion (in context). Anterolateral leads here would be described as pseudo-normalization (because the context tells us they are NOT normal, they are transitioning from reperfusion TWI to acute anterolateral active OMI with T waves reinflating into hyperacute T waves, if the occlusion persists). This does NOT happen in myocarditis!! |
It sounds as if the pain suddenly ceased, and no more ECGs were ordered for days.
5,040 ng/L
3,933 ng/L
2,517 ngL
1 week later:
 |
| Mostly all areas show reperfusion, except inferior leads. |
The patient was initiated on guideline-directed medical therapy for his HFrEF, atorvastatin and clopidogrel for his MI, and warfarin for the LV thrombus. He was discharged on hospital day 14 following recovery from COVID pneumonia complicated by an anterior OMI.
Final diagnoses:
"STEMI vs Pericarditis in context of HFrEF
LV thrombus 2/2 myocardial hypokinesia s/p STEMI v Pericarditis"
1 month later:
 |
| Still showing reperfusion. |
Months later:

A cardiac MRI was performed outpatient 4 weeks following the hospitalization. The imaging demonstrated a mid-apical inferoseptal and apical reversible defect consistent with infarct provided below.

Unfortunately, the patient has experienced multiple complications since discharge requiring recurrent hospitalizations due to UGIBs in the setting of anticoagulation and antiplatelet agents. This case highlights the importance of timely intervention with PCI for OMI in order to reduce the incidence of post-MI complications and the complications from medical management.
Learning Points:
In this case, the patient's management disagrees with both the current ACC/AHA NSTEMI guidelines which give a 1A recommendation for emergent cath for NSTEMI with ongoing ischemia, as well as the 2020 AHA statement on myocarditis, which states:
"A nonvascular distribution of ST-segment elevations is common in fulminant myocarditis but should not delay angiographic assessment of the coronary anatomy." Also: "Although an elevated serum cardiac troponin (cTn) is almost always present in fulminant myocarditis, there should be a low threshold for evaluation with coronary angiography because acute coronary syndrome is the most common cause of a cardiac presentation with elevated biomarkers."
Myocarditis and takotsubo cardiomyopathy can closely mimic OMI. In some cases, the ECG cannot differentiate these conditions. However, myocarditis should not mimic the OMI progression including reperfusion and reocclusion, as we saw in the case above. With myopericarditis having a much lower incidence than OMI and the consequence of missing an OMI being severe, having a low threshold for early angiography is an appropriate approach to diagnostic evaluation.
Myocarditis and takotsubo cardiomyopathy can closely mimic OMI. In some cases, the ECG cannot differentiate these conditions. However, myocarditis should not mimic the OMI progression including reperfusion and reocclusion, as we saw in the case above. With myopericarditis having a much lower incidence than OMI and the consequence of missing an OMI being severe, having a low threshold for early angiography is an appropriate approach to diagnostic evaluation.
Clinical context and ancillary tests other than the ECG can help differentiate these conditions. This patient had features including rapidly rising troponin and focal wall motion abnormality, both of which should of course be considered due to OMI until proven otherwise. Myocarditis as a cause of this case can only be entertained after emergent angiogram. An emergent coronary CT angio would also be a reasonable plan for a patient for whom the diagnosis of OMI is in doubt due to possible myocarditis or takotsubo. This cardiologist seems to be able to ignore almost any possible clinical feature, but imagine if the primary team had obtained CT coronary angio showing occlusion or high grade stenosis of the LAD.
A case series from the NEJM (Bangalore et al., in references below), further highlights the difficulty in discerning OMI from myopericarditis in COVID-19 patients. This series identified 18 patients with COVID19 who presented with ECG features suggesting STEMI. Following additional evaluation, 8 patients were determined to have OMI and 10 patients were determined to have non-coronary myocardial injury. The ST segment elevation was identified as diffuse in 4/10 of the non-coronary myocardial injury cases and focal in 6/10 of the non-coronary myocardial injury cases. This series emphasizes the lack of specificity of ST segment changes and distribution in distinguishing OMI from myo-pericarditis.
Many patients will unfortunately present with vague symptoms that cannot be used to confidently discern these two pathologies. Laboratory evaluation using a CRP/troponin ratio may provide some additional insight. A CRP/troponin ratio >500 was found to have an 85% specificity for myopericarditis and >1000 has a 92% specificity for myopericarditis. The consequence of missing an OMI, however, is exceptionally high and using the CRP/troponin ratio as the sole reason to defer cardiac catheterization is risky. Better to consider myocarditis as a diagnosis that is only possible to make after the angiogram and other features rule out OMI.
References:
Bangalore S, Sharma A, Slotwiner A, et al. ST-segment elevation in patients with COVID-19 – a case series. New England Journal of Medicine. June 2020; 382: 2478-2480. https://www.nejm.org/doi/full/10.1056/NEJMc2009020
Bangalore S, Sharma A, Slotwiner A, et al. ST-segment elevation in patients with COVID-19 — a case series; Supplementary appendix. New England Journal of Medicine. 2020; 382:2478-80. https://www.nejm.org/doi/suppl/10.1056/NEJMc2009020/suppl_file/nejmc2009020_appendix.pdf
Circulation 2020: ACC/AHA Statement on Management of Fulminant Myocarditis:
https://www.ahajournals.org/doi/10.1161/CIR.0000000000000745
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0248365
===================================
MY Comment, by KEN GRAUER, MD (7/25/2022):
===================================
Brilliant discussion of today's case by Dr. Parker Hambright — with contributions from Drs. Meyers, Smith and McLaren. At the risk of repetition — I'll reemphasize KEY points brought out regarding the distinction between acute OMI vs Myocarditis.
- By itself, the initial ECG can not reliably distinguish between acute OMI vs Myocarditis. There is simply too much overlap of ECG findings between these 2 entities to provide a definitive diagnosis based on a single tracing.
- Use of serial ECGs may faciliate distinction — as was seen in today’s case with the appearance of reperfusion T waves. Unfortunately, this ECG finding was not seen until ECG #7 (done on Day-3 at 12:10) — at a time that was well beyond that likely to provide benefit from PCI.
- Long before the "tell-tale" ECG sign of reperfusion T waves — presumptive diagnosis of acute OMI until you prove otherwise was evident from focal evolution of ECG findings (recognized as soon as ECG #2 became available to compare with ECG #1).
- Bedside Echo provided further support of focal injury (serving as an additional indication to assume acute OMI until you prove otherwise).
- Cardiac MRI could distinguish between OMI vs Myocarditis — but this modality will not be available to many (most) providers in a timely-enough fashion to positively impact treatment.
- BOTTOM Line: As emphasized above by Drs. Hambright, Meyers, Smith & McLaren — there are times when cardiac catheterization may be the only way to definitively distinguish between OMI vs Myocarditis. The clinical lesson is to expedite identification of which patients need prompt cath — because we recognize that without prompt cath, we simply may not be able to distinguish between acute OMI vs Myocarditis in problematic cases.
What Happened in Today's Case:
Unfortunately — the diagnosis of acute OMI was significantly delayed in today's case because of oversights pointed out above in Dr. Hambright's discussion. To facilitate appreciation of these oversights — I thought it worthwhile to take another LOOK at the first 2 tracings in today's case (Figure-1):
-USE.png) |
| Figure-1: Comparison between the first 2 tracings in today’s case (See text). |
Comparing the 2 ECGs in Figure-1:
The point I would emphasize about ECG #1 — is that this is not a "normal" tracing. I completely agree with Dr. Hambright that the subtle-but-real ST depression in at least 6 leads (with hint of ST elevation in lead aVR) — is consistent with diffuse subendocardial ischemia (which is not unexpected given the clinical context of Covide-related acute respiratory failure).
- I'd add that while not depressed — the ST segment in lead V2 of ECG #1 is abnormally straightened — with angulation at the point that it joins the T wave. Considering modest size of the QRS complex in this lead — I thought the T wave in lead V2 was taller-than-expected, and in the context of the straightened ST segment — possibly hyperacute.
- Given the association of severe Covid illness with acute cardiac disorders (such as myocarditis and OMI) — these ECG findings in this initial tracing (even in the absence of chest pain at this time) would seem to merit: i) Ordering troponin (which was not done in today's case until after ECG #2); and, ii) Repeating the ECG much sooner than was done (ECG #2 was not done until 11 1/2 hours later — and then only because the patient had chest pain).
- I can't help but wonder if that overly tall T wave in lead V2 of ECG #1 might had heralded the beginning of this patient's LAD occlusion.
I chose to put ECGs #1 and #2 together in the same Figure-1 — because the changes that occurred between these 2 tracings are so striking. Almost every lead shows evolution!
- Whereas the "amount" of ST elevation in the inferior leads of ECG #2 is not great — this most definitely is a dynamic ST-T wave change when you consider how flat the ST segments were in ECG #1.
- Although the QRS in lead aVL of ECG #2 is tiny — the change from an upright T wave in this lead in ECG #1 — to a negative ST-T wave in ECG #2 is a real indication of reciprocal change.
- The amount that the ST segments in leads V3 and V4 of ECG #2 have elevated — is even more than what one might think when you factor in the starting point of ST depression in these leads that was present in ECG #1.
- Even the flat ST segments in leads V5,V6 of ECG #2 represent some elevation of ST segments considering the ST depression that was present in ECG #1.
The conclusion from comparing ECG #2 with the initial tracing in today's case is compelling:
- The patient has severe Covid-related illness. He is therefore predisposed to acute cardiac disorders such as myocarditis and OMI. The onus of distinguishing between acute myocarditis vs OMI is on us.
- While a single ECG by itself might not be able to reliably distinguish between these 2 entities — the patient has new chest pain and has clearly evolved focal ST elevation with dynamic ST-T wave changes in multiple leads.
- BOTTOM Line: It was OK not to be 100% certain at this point in the case as to whether the patient had acute myocarditis or acute OMI (neither Echo nor troponins were yet done). Regardless — it should have already been evident that prompt cardiac cath was needed for definitive diagnosis (since you otherwise will not be able to rule out acute OMI).
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.