
Written by Jesse McLaren
Two patients presented with chest pain and LVH on ECG.


Do STEMI criteria help?
Both have
anterior STE in two contiguous leads that exceed STEMI criteria, but both also have
LVH. LVH produces tall R waves in the left
sided leads with secondary ST depression and T wave inversion, and deep S waves
in the right sided leads with secondary ST elevation and tall T waves. In the first patient the left sided leads don't have very tall R waves, but they do have deep right sided S waves.
Because STEMI criteria only looks at amplitude of ST elevation, it can’t differentiate between secondary and primary or superimposed causes of ST elevation, and ignores other signs of acute coronary occlusion. Instead the paradigm simply defines STEMI as ST elevation in the absence of LVH. So by definition STEMI criteria cannot be applied to these ECGs, and cannot identify which has acute coronary occlusion. Armstrong suggested using a cutoff of STE/S > 25%, but this would call both of these negative: in the second case V3 has an S wave of 28mm, which would require 7mm of STE and there’s only 4. (see this post for further discussion)
Do old ECGs help?
Here are the two cases with the old followed by the new ECG:
Patient 1:

If you only looked at ST segments and T waves you might be concerned about increase ST elevation and taller T waves in V1-2, but these are proportional to larger voltages in those leads. LVH can change over time, and can also be affected by lead placement: the older ECG has higher leads, with almost entirely negative P wave in V1 and biphasic P in V2. On the other hand, the prior ECG does show that the inferolateral T wave inversions are old, and they remain asymmetric and proportional to the QRS complex. So the new ECG shows LVH with secondary repolarization changes, without ECG evidence of OMI.

The new ECG has greater STE in V1-3 with the same voltages, but also multiple other signs of OMI: 1) while the Q waves V1-3 are old there is loss of R wave in V4, 2) there are hyperacute T waves V3-4, and 3) there’s inferolateral ST depression especially in V5-6, which is reciprocal to anterior ST elevation. (Compare the typical LVH strain pattern from patient 1 with asymmetric T wave inversion, with ischemic reciprocal change in patient 2 with ST depression with upright T wave).
How were they managed? STEMI criteria fails to identify occlusion and reperfusion
Patient 1 had serial ECGs that were unchanged and serial troponin which were normal (4 and 5 ng/L, with normal < 16 in females and <26 in males). They were discharged and well on follow up.
Patient
2 had three sprays of nitro with improvement of symptoms. Here is the first ECG
and repeat:

This was interpreted as resolution of ST changes, and with an initial troponin of 13ng/L the patient was observed with a plan for non-urgent angiogram based on "transient STEMI". But notice there’s been a total loss of R wave in V4, there is still a hyperacute T wave, and there is ongoing inferolateral ST depression. Despite improvement of symptoms there’s been no reperfusion.
Four hours later a repeat troponin was 3500ng/L and another ECG was done, with the patient reporting more pain:

There are still hyperacute T waves V3-4 and still inferolateral ST depression, and now more ST elevation V3-4. Cath lab was activated, after hours of preventable infarction, and found what the first ECG revealed: proximal LAD occlusion. While the first troponin was in the normal range, the peak was 33,000ng/L. Discharge ECG showed precordial T wave inversion, indicating reperfusion:

Take away
1. LVH produces secondary ST and T wave changes that can vary over time
2. STEMI criteria is defined in absence of LVH so can’t help identify OMI in the presence of LVH
3. Other signs of OMI include loss of R waves, disproportionate ST elevation, hyperacute T waves, and reciprocal ST depression
4. Resolution of symptoms is not the same as reperfusion, and resolution of ST segments is not the same as reperfusion T wave inversion
5. Initial troponins can be normal, symptoms can resolve and patients can have "transient STEMI" all in the presence of ongoing OMI and relying on these features can lead to delayed reperfusion
![]()
===================================
MY Comment, by KEN GRAUER, MD (7/29/2022):
===================================
- In the hope of providing additional perspective to the 2 insightful case studies described above — I focus my comments on some non-numeric "qualitative" features that have been helpful to me.
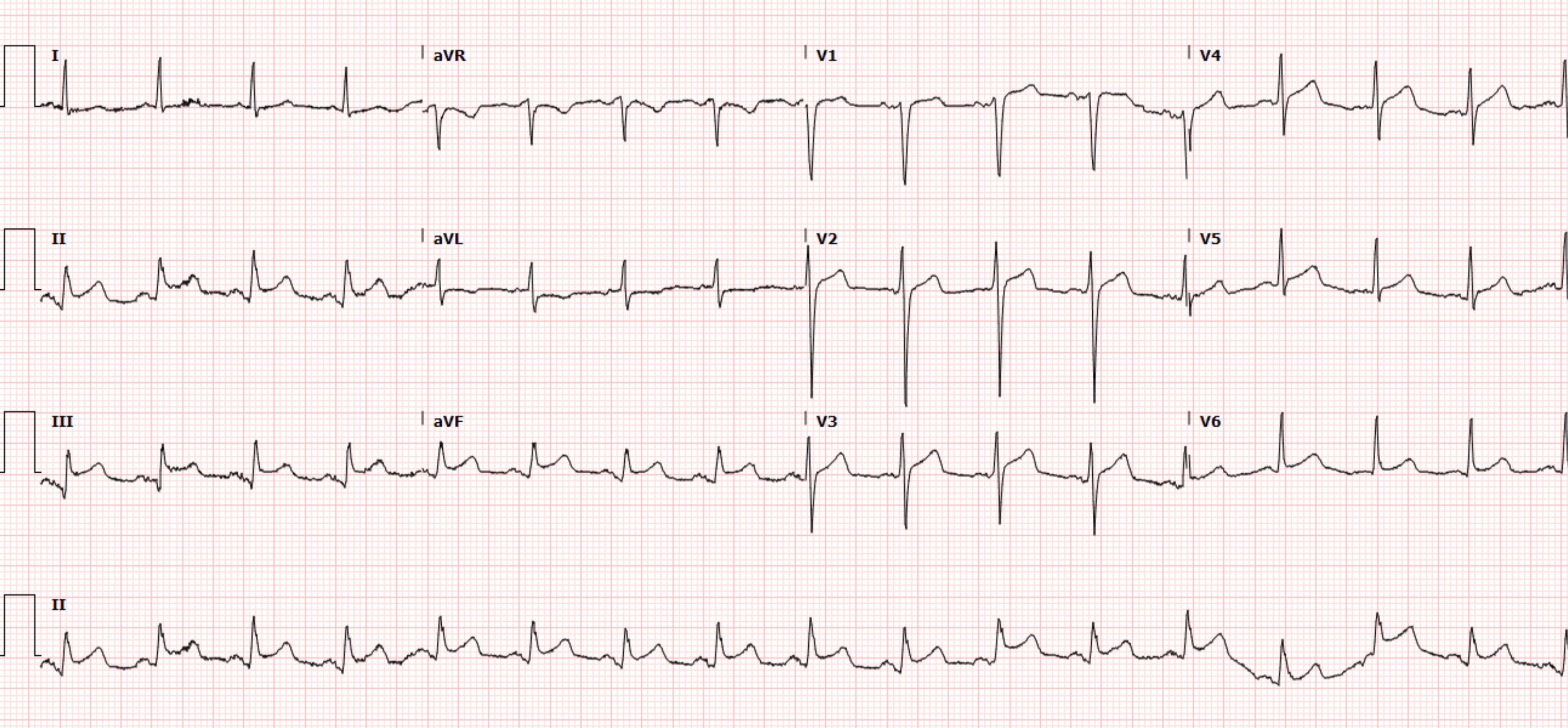
- To illustrate these features — I've reproduced and labeled in Figure-1 the initial ECG from Dr. McLaren's Patient 2 ( = the 2nd ECG shown above).
- Since reliable numeric criteria do not exist for identifying acute OMI in patients with marked LVH — we need to focus our attention on other clues. The "essence" of applying the factors of Shape — Proportion — Location — is that we are looking for QRST morphology changes "that should not be there".
- Textbook criteria for this do not exist. Instead — we intuitively use our "memory banks" of all the hundreds (thousands, or more) tracings we've interpreted over our years of practice — to arrive at a conclusion of relative probability that an ECG in a patient with baseline LVH and new symptoms is (or is not) likely to be evolving an acute cardiac event.
- I favor starting by search for those 1 or 2 leads on the 12-lead tracing for which I can be fairly certain that QRST appearance in a patient with new symptoms is not "normal".
- I then look at "neighboring leads" — to see if less obvious changes are likely to reflect a "continuation" of suspected acute changes.
- In general — the more leads with suspected acute changes on a 12-lead ECG — the greater the likelihood that an acute process is evolving.
- In Dr. McLaren's above discussion — he illustrates how additional information (ie, comparison with prior and/or serial tracings; troponin values; correlation with the patient's clinical response to treatment) — may assist for identifying which LVH tracings show an acute process. But initially, before this additional information becomes available — we are often faced with assessing the situation from only the initial ECG.
-USE.png) |
| Figure-1: I've reproduced the 2nd ECG shown in Dr. McLaren's above discussion — which was the initial tracing obtained in the ED from his Patient 2. |
- There is marked baseline artifact in the limb leads. Despite this — the tracing is interpretable.
- The rhythm is sinus at ~75/minute. All intervals and the mean QRS axis in the frontal plane are normal.
- There is marked LVH (very deep S wave in V3>25 mm; very tall R waves in V5,V6 greater than 30 and 20 mm, respectively).
- There are QS complexes in leads V1,V2,V3.
- Transition is slightly delayed — with the R wave becoming taller than the S wave is deep between leads V4-to-V5.
- The most remarkable ECG findings are the ST-T findings (See below).
- Not all patients with Echo-proven LVH manifest LV "strain" on ECG. The Framingham Studies taught us that longterm prognosis is adversely affected when both voltage and repolarization changes of "strain" are present on ECG.
- ST-T wave changes of LV "strain" are most commonly seen in one or more of the lateral leads (ie, in leads I, aVL; and/or V4, V5, V6). Typically — there is slow descent of the ST segment, with a more rapid rise at the end of the ST segment.
- Some patients with LVH (especially if the frontal plane axis is vertical) — also manifest ST-T changes of LV "strain" in the inferior leads.
- Some patients with especially deep anterior S waves — manifest the "mirror-image" picture of LV "strain" in the form of an upright ST-T wave, often with some ST elevation in these anterior leads.
- The other major effect produced by LVH on ECG is that the increase in leftward and posterior forces forces may overshadow baseline anterior forces — with a "net result" that R wave progression is delayed (sometimes to the point of producing QS complexes in one or more anterior leads).
- NOTE: I've reviewed my approach for ECG assessment of LVH and LV "strain" on many occasions in Dr. Smith's ECG Blog (For more — SEE My Comment in the June 20, 2020 post and the April 27, 2019 post — to name just 2 of these posts).
- Although there is a QS complex in anterior leads V1,V2,V3 — I was not certain from this single tracing if this was the result of anteroseptal infarction at some point in time — or — simply a reflection of predominant leftward and posterior forces from marked LVH that resulted in elimination of all anterior R wave. The fact that the small QRS complex in lead V4 was isoelectric (outlined in BLUE in Figure-1) — and then followed by a dramatically tall R wave in lead V5 suggested to me that the QS complexes in anterior leads were probably the result of LVH.
- Following my suggested approach to LOOK FIRST for those 1 or 2 leads in which I could be fairly certain that the ST-T waves were "not normal" — I focused on the T wave in lead V4. Although this V4 lead clearly represents a "transition lead" between the markedly negative QRS in lead V3 — and the markedly positive QRS in V5 — in this 70-year old with new chest pain, I thought there was NO way the T wave in lead V4 could be normal. This T wave is pointed, more than twice as tall as the R wave in this lead — and manifests a wide base. In a patient with new symptoms — I interpreted this T wave in lead V4 as hyperacute until proven otherwise!
- Moving on to "neighboring leads" — while the initial part of the depressed ST segments in leads V5 and V6 (outlined in RED) could be consistent with LV "strain" — there was NO way the tall, pointed terminal T wave positivity in lead V5 could be normal. As a result — I thought the small, but still unusually pointed terminal T wave positivity in lead V6 was probably further extension of the same ongoing process.
- The other "neighboring lead" to the hyperacute T wave in lead V4 — was lead V3. And while common with markedly increased anterior S waves from LVH to see fairly tall, upright ST-T waves in those anterior leads with increased voltage — the 15 mm tall, pointed T wave in lead V3 (outlined in BLUE) closely resembles the appearance of the hyperacute T wave in lead V4.
- The T wave in lead V2 (outlined in BLUE) looks hypervoluminous with respect to the relatively small QRS in this lead.
- The ST segment in lead V1 is elevated and abnormally coved (almost a "reciprocal" mirror-image picture of the scooped ST segment depression in lateral chest leads V5,V6).
- Subtle ST-T wave flattening is seen in limb leads III and aVF. Although this is a nonspecific change — I thought the shape of the ST-T wave in lead II (outlined in BLUE) in association with unexpected J-point depression in this lead (RED arrow) — was clearly abnormal.
- Virtually all leads on this tracing showed abnormalities beyond that expected for simple LVH — and, given the history of new chest pain — I was suspicious of hyperacute ST-T waves in all 6 chest leads.
- I thought chest lead T waves (especially in leads V3-thru-V5) had a deWinter-like appearance — so despite marked LVH — I thought, "acute proximal LAD occlusion" until proven otherwise.













-USE.png)






-USE.png)
