
Case written by Neha Ray, MD, with edits by Meyers, Smith, Grauer
A woman in her 50s presented for evaluation of multiple episodes of syncope with shortness of breath. On EMS arrival, she was GCS 15 with HR 110s. En route to the ED, the patient had 4 more episodes of syncope and became hemodynamically unstable with SBP in the 80s and HR 160s. The first recorded SpO2 was 73%. On arrival to the ED, patient was diaphoretic and in extremis. Her initial EKG is below. Paramedics arrive to the ED and state that they are worried about inferior STEMI.
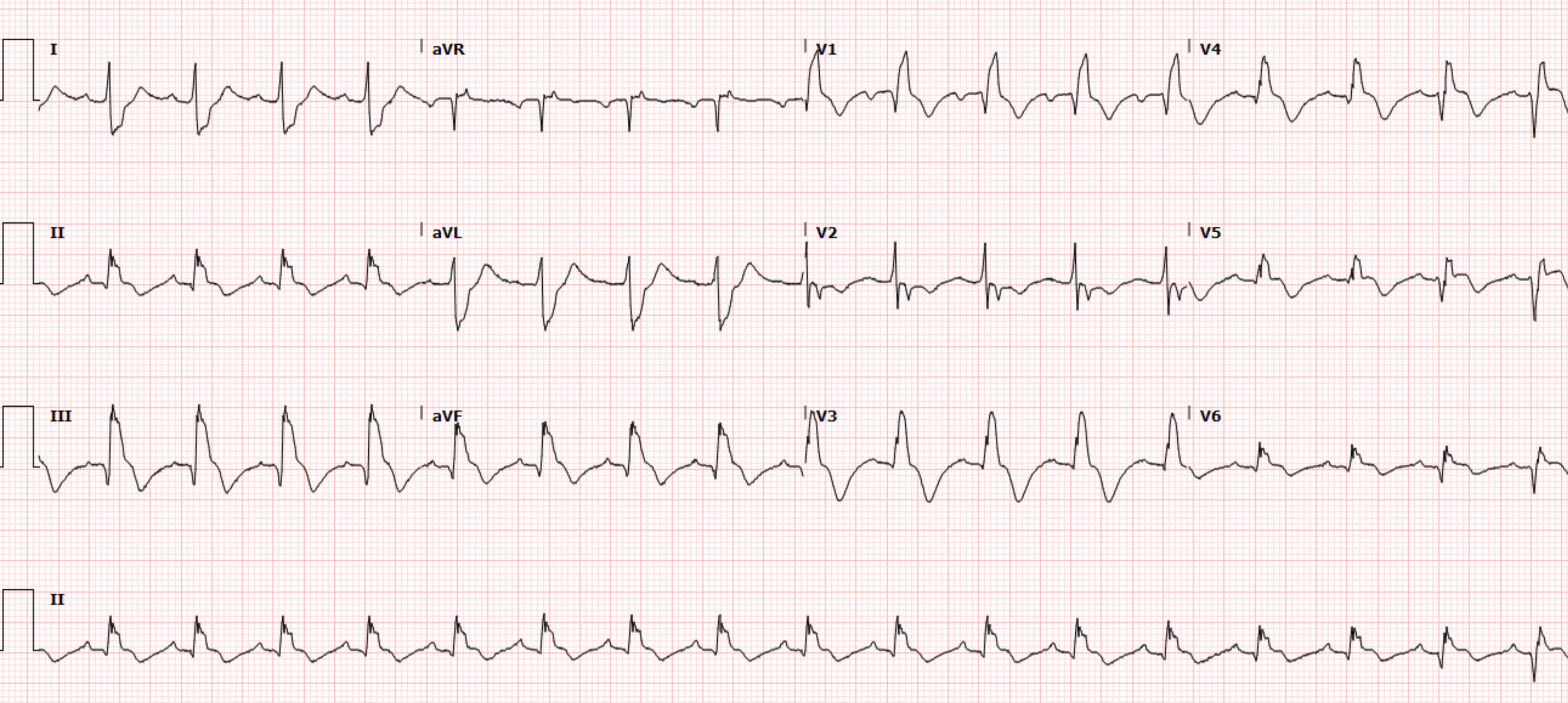
What do you see?

The ECG shows sinus tachycardia with prominent T-wave inversions in the inferior and anterior leads. The patient also has right axis deviation, and an S1Q3T3 pattern. There is a hint of inappropriate STE in III, with reciprocal STD in I and aVL.
It would be easy to mistake this ECG for inferior OMI (STE in III with reciprocal STD in aVL). But several features give it away as a mimic of OMI and instead all but diagnostic of right heart strain. Most important is tachycardia, which should always make you doubt the diagnosis of OMI. When there is tachycardia, there is either OMI with cardiogenic shock (which should have poor LV function on echo or valvular dysfunction) or there is another etiology. T-waves: 1) when inverted in both anterior and inferior leads, PE is far more likely than ACS. 2) Domed T-wave inversion 3) T-wave inversion during pain, in contrast to post-pain, as seen in reperfusion and Wellens syndrome.
While no prior was available, the providers correctly identified findings consistent with acute right heart strain. A beside TTE was performed, see images below.
The TTE shows a dilated right ventricle with D-sign on the parasternal short view. On the apical 4 view, you can see septal bowing and McConnell’s sign (right ventricular free wall akinesis with apical sparing). The IVC also appeared plethoric concerning for elevated right atrial pressure. While RV dilation with D-sign and elevated RAP can occur in both acute and chronic right heart strain, McConnell’s sign is more specific for acute pulmonary embolism (though data is conflicting). The providers performed a lower extremity US showing a left popliteal vein DVT, further confirming the diagnosis of acute massive PE. The patient was given an initial 10 mg bolus of alteplase.
Shortly after this, and 15 minutes after the initial ECG, the patient develops agonal breathing and has a PEA arrest. Patient is administered and additional 40 mg of alteplase and ROSC is obtained. The patient was placed on an epinephrine drip and intubated. Her repeat ECG post-ROSC is shown here:
This ECG shows continued sinus tachycardia, persistent T-wave inversions in the inferior and anterior leads with an S1Q3T3 pattern. However, the patient has also developed a new complete right bundle branch block, thought to be predictive of more severe pulmonary hypertension. There is also concordant STE in III and aVF, with reciprocal STD in I and aVL. This is likely due to an element of type 2 STEMI or type 2 OMI pattern which can occur when massively increased demand outstrips very low supply to the point that the supply/demand mismatch effectively resembles the same physiologic state as OMI, with transmural injury.
The patient has another brief arrest during which she received an additional 50 mg of alteplase, but is ultimately is taken to CT scanner which demonstrates pulmonary emboli in the main pulmonary arteries bilaterally with elevated RV/LV ratio.


She is admitted to the ICU and undergoes pulmonary artery aspiration thrombectomy. After a prolonged hospital stay, she is ultimately able to be discharged home with intact neurologic function.
First troponin I on arrival was 91 ng/L (upper reference limit for women 12ng/L for this assay). No further troponins were ordered.


A crashing patient with an abnormal ECG that you must recognize
Chest pain, ST Elevation, and tachycardia in a 40-something woman
Learning Points:
Pulmonary embolism is overall rare in patient’s presenting with syncope, with an estimated prevalence <1%. However, syncope in the setting of PE has been shown to have higher 30-day mortality compared to patient with PE without syncope. In this patient, quick identification of abnormal ECG and bedside US findings allowed for a life-saving resuscitation.
You must learn this acute right heart strain pattern if you want to save these lives.
Type 2 STEMI or OMI patterns occur in situations with severely mismatched regional supply and demand. The affected myocardium experiences the same transmural injury regardless of the etiology.
References:
1. Mcconnell MV, Solomon SD, Rayan ME, Come PC, Goldhaber SZ, Lee RT. Regional right ventricular dysfunction detected by echocardiography in acute pulmonary embolism. Am J Cardiol. 1996;78(4):469-73.
2. Avila J. Is McConnell’s sign useful for APE? 5 minute sono - 5 Minute Sono Blog. https://blog.5minsono.com/mcconnells-sign/. Accessed March 2, 2022.
3. Petrov DB. Appearance of right bundle branch block in electrocardiograms of patients with pulmonary embolism as a marker for obstruction of the main pulmonary trunk. J Electrocardiol. 2001 Jul;34(3):185-8. doi: 10.1054/jelc.2001.25132. PMID: 11455507.
4. Prandoni P, Lensing AW, Prins MH, et al. Prevalence of Pulmonary Embolism among Patients Hospitalized for Syncope. N Engl J Med. 2016;375(16):1524-1531. PMID: 27797317
5. Roncon L et al. Impact of Syncope and Pre-Syncope on Short-Term Mortality in Patients with Acute Pulmonary Embolism. Eur J Intern Med 2018; 54: 27-33. PMID: 29655808
MY Comment, by KEN GRAUER, MD (3/28/2022):
===================================
- Q waves, ST elevation and T wave inversion in leads III and aVF.
- ST depression in leads I and aVL.
- Chest lead T wave inversion.
-USE.png) |
| Figure-1: The first 2 ECGs in today’s case (See text). |
It’s easy to understand how the EMS team might have thought this acutely ill patient was having an acute infarction. That said — there are a series important clues that taken together, should immediately prompt emergency providers to consider a large acute PE (Pulmonary Embolus) as the diagnosis until proven otherwise.
- Fortunately, ED (Emergency Department) providers quickly recognized the correct diagnosis — and promptly initiated appropriate therapy. Despite this — the patient experienced a PEA arrest. As per Drs. Ray and Meyers — the patient was successfully resuscitated.
The 1st big CLUE to the correct diagnosis in today’s case is the History. This patient did not present with chest pain. Instead, this woman in her 50s had multiple episodes of syncope associated with shortness of breath.
- In the context of this clinical history — the initial ECG should strongly suggest the diagnosis of a large acute PE until you prove otherwise. In my experience — syncope caused by acute PE is a potentially ominous sign — especially given the multiple recurrences of this symptom in today’s case.
- As emphasized by Drs. Ray and Meyers — prompt ordering of Stat Echo at the bedside allowed confirmation of acute massive PE within the space of a few minutes! The value of Stat Echo in the ED for confirming our clinical and ECG suspicion of acute PE cannot be overstated!
What is it about ECG #1 that Suggests a Large Acute PE?
- Sinus Tachycardia: While not absolutely essential for the diagnosis, a rapid heart rate (usually to at least 90/minute) is a common and expected finding in patients with hemodynamically significant acute PE. The heart rate in today’s case is extremely rapid! (ie, at ~135/minute in ECG #1).
- S1Q3T3: In my experience, it is rare (if ever) that the isolated finding of an S1Q3T3 pattern will make the diagnosis of a new significant PE. That said, this ECG sign may be extremely helpful IF seen in association with other ECG evidence of acute PE. Such is the case in today’s tracing.
- Acute RV “Strain”: Awareness of ECG evidence of RV (Right Ventricular) "Strain" is one of the most important ECG indicators of acute hemodynamically significant PE. Unfortunately, this sign remains all-to-often unappreciated and misinterpreted as coronary ischemia. RV “strain” manifests as ST depression and/or T wave inversion that typically occurs in anterior leads (V1,2,3) — and/or — in inferior leads (II,III,aVF). Abnormal ST-T wave changes consistent with this finding are seen in both of these lead areas in ECG #1.
- NOTE #1: There is something about lead V2 in ECG #1 that is “off”. The much larger QRS amplitude and different morphology seen in lead V2 (compared to QRS morphology in neighboring leads) just does not make physiologic sense. The lack of the symmetric T wave inversion in lead V2 is also incongruous with the picture we see in other chest leads (ie, T wave inversion begins in lead V1 — and becomes quite marked in leads V3, V4, V5). Precordial lead electrode placement should be verified on future ECGs.
- NOTE #2: The “shape” of the coved ST segments that lead into deep symmetric T wave inversion with an associated prolonged QTc interval in both inferior and chest leads presents a picture that “looks” more typical in morphology of RV “strain” than of acute MI from coronary occlusion.
- RAA (Right Atrial Abnormality): RAA is another ECG indicator of acute right heart strain. RAA is most often diagnosed by the finding of a tall, peaked and pointed P wave (≥2.5 mm) seen in one or more of the inferior leads. Less commonly — RAA may be suggested by the finding of a pointed upright P wave in lead V1 and/or V2. Even though amplitude of the P wave seen in lead II may not quite attain a height of 2.5 mm — the multiple P waves seen in the artifact-laden long lead II are definitely “pointed” — to in my opinion, diagnostic of RAA. Given that the only condition in medicine known to enlarge the RA without also enlarging the RV is tricuspid stenosis — recognition of RAA in today’s tracing carries important diagnostic value.
- The Abnormal Frontal Plane Axis: Reference is often made to RAD (Right Axis Deviation) as a sign of acute PE. But in addition to RAD — an indeterminate frontal plane axis carries similar diagnostic value. RAD is not present in ECG #1 — because the QRS complex is not predominantly negative in lead I. Instead — the QRS complex is nearly isoelectric in each of the 6 limb leads — which defines the frontal plane axis as indeterminate, adding further support to the diagnosis of acute RV "strain".
- Poor R wave Progression: Note persistence of sizeable S waves across the precordium (ie, the finding of fairly deep S waves in leads V5 and V6 suggests significant forces away from these left-sided leads — which in this tracing means there is probably an increase in right-sided forces).
- Among the unappreciated benefits of lead aVR in ECG interpretation, is awareness that acute right heart “strain” (as seen with large acute PE) may often produce ST elevation in right-sided lead aVR. Although subtle — there is ST elevation in lead aVR in ECG #1. A similar pattern of ST elevation may also be seen in right-sided lead III.
-USE%20copy.png) |
| Figure-2: ECG findings associated of acute PE. There is no single ECG finding that is diagnostic of acute PE. Instead, the diagnosis may be suggested by the presence of at least several of these ECG findings when they occur in the “right” clinical setting (See text). |
NOTE: The ECG is far less likely to help in the diagnosis of relatively small (ie, subsegmental) PEs that are not hemodynamically significant, and which are often only discovered on Chest CT performed on patients with less convincing symptoms. This is probably a “good thing” — since evidence is lacking that treatment of incidentally discovered, non-hemodynamically significant subsegmental PEs is beneficial (and it certainly is not without potential for harm). Perhaps it is a “benefit-in-disguise” that the ECG is unlikely assist in detection of relatively smaller pulmonary emboli.
-----------------------------------------------------------
Drs. Ray and Meyers expand on the likelihood of a Type 2 STEMI (due to severely mismatched supply-demand) as the reason for the findings we see with ECG #2 (as shown in Figure-1 above).
- It should be noted that we were already seeing the beginning of these changes in the limb leads of ECG #1 (ie, Q waves, ST elevation and T wave inversion in leads III, aVF — with mirror-image ST depression in leads I and aVL).
- Otherwise, as mentioned above — there is now complete RBBB (Right Bundle Branch Block).
- Once again — something about lead V2 doesn’t “fit”, because of how different QRST morphology in lead V2 of ECG #2 looks compared to QRST appearance in each of the other 5 chest leads. Since ECG #2 was also obtained in the ED, not long after ECG #1 — I suspect the same person may have recorded both of these initial 2 ECGs (potentially committing the same lead V2 electrode placement error).
- Confession: If I would have been shown ECG #2 alone, without information about the clinical history — I would probably have diagnosed acute or recent STEMI, possibly in the reperfusion T wave stage. After all, there are inferior lead Q waves plus small-but-real q waves in multiple chest leads. And in each of these leads with Q waves — there remains some ST elevation with surprisingly deep T wave inversion well beyond that expected from the RBBB.
- KEY Point: More than just development of RBBB on this post-ROSC tracing — is the QR morphology in lead V1. In patients with mitral stenosis from rheumatic heart disease — this ECG finding is highly predictive of markedly elevated pulmonary pressure. There is a physiologic reason why pulmonary hypertension from advanced mitral stenosis commonly results in a qR pattern in lead V1 (Figure-3). Given the "D-shaped" deformity on Echo in today's case — I think it highly likely that the same physiology applies in this patient with massive acute PE and associated pulmonary hypertension.
 |
Figure-3: With permission, I've adapted Figure-2 from a slide sent to me by Dr. Balasubramanian (from Pondicherry, India). — LEFT: The circular configuration of the normal left ventricle in this short-axis view — with corresponding rS morphology in lead V1 (WHITE arrow illustrating septal depolarization that is initially oriented toward lead V1). — RIGHT: Increased RV pressure (with associated RV dilatation) is transmitted to the interventricular septum, and produces a "D-shaped" deformity of the LV (as seen here, in this short-axis view). Flattening of the septum in this manner alters the direction of initial septal activation, that is now oriented away from lead V1 (WHITE arrow), thereby producing the qR pattern in lead V1 that is seen with RVH + pulmonary hypertension. |
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.