
This was written by @BrooksWalsh, with one comment by Smith
A middle-aged guy comes in with chest pain. No known cardiac disease, and he’s healthy enough that he was hiking in some hilly terrain when he developed the symptoms..
He comes into the ED, and they get an ECG which shows…
He comes into the ED, and they get an ECG which shows…

… and is read by the computer as:

Very reassuring, especially in the context of evidence that a computer interpretation of “normal” is “unlikely to have clinical significance that would change triage care.”
(HINT: this paper is very flawed, as Litell, Meyers and Smith point out in this article:
Also, the troponin (not high-sensitivity) is undetectable, so is this guy is ready for d/c, amirite?
Emergency physicians should be shown all triage ECGs, even those with a computer interpretation of "Normal"
Also, the troponin (not high-sensitivity) is undetectable, so is this guy is ready for d/c, amirite?
“Not so fast” you say?
For starters, it would be reasonable to ask how soon after symptom onset the troponin was drawn - it was within 1-2 hours, a bit too soon to use a single marker. Also, perhaps serial ECGs would be preferred? Ah, we’ll get to that later.
But first, long-time readers of this blog are unlikely to fall for the “Computer said the ECG was normal” ploy. But you can’t call out the cath team based on reverse psychology, so let’s take a closer look at the ECG!
Close up of ECG
Scrutinizing the ECG, we can see that there’s some subtle ST segment elevation in leads III and aVF.
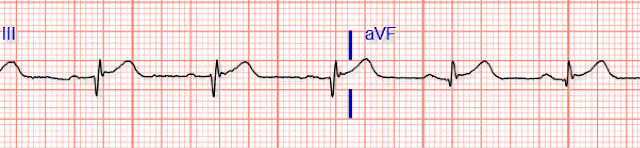
The ST elevation is mild, though, < 1 mm in both leads. And of course this can happen in pericarditis, say, or early repolarization.
However, what should raise some concerns is the ST segment in the oft-neglected aVL:
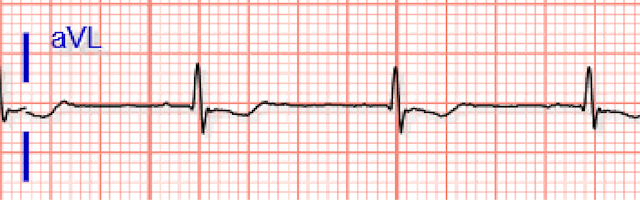
Looks like a bit of ST depression here, and while it isn’t a lot, it’s all we need! In the context of inferior STE, if there is any STD in aVL then pericarditis is almost completely ruled-out, and acute coronary occlusion is very likely!
Smith comment: in the context of a presentation compatible with ACS, this so-called "normal" ECG is DIAGNOSTIC of inferior Occlusion MI [This is a STEMI (-) OMI as it does not meet 1 mm STEMI criteria]. It can't be anything else. Activate the cath lab, don't wait for the troponin and, if you do, ignore it if "negative."
Continued
About those serial ECGs…
A doctor with a keen eye noted the subtle STD in aVL, and called out the troops (not the trops).
A doctor with a keen eye noted the subtle STD in aVL, and called out the troops (not the trops).
A second ECG was a bit more flagrant!

Even more diagnostic of inferior OMI
Resolution
Following the expeditious placement of a stent in the right posterior descending artery, the patient recovered quite nicely. Some corresponding regional hypokinesis was found on echo, and a follow-up ECG showed some inferior Q waves.

Had the initial ECG led the clinicians to label this as a “non-STEMI,” however, things might not have evolved so well - let alone if he had been discharged!
Here are 29 other posts in which the computer made a grave error of "normal ECG":
Yet another great example of the importance of STD in aVL in the setting of inferior STE!
ReplyDeleteHoweever, I think the inferior Q waves didn't only show up in the last ECG; they were there all along since the first one (although not wide, Q/QRS ratio is definitely likely to result from an ischemic myocardial inury). It somehow puzzles me how they seem to disappear (or at least look a lot less "ischemic") in the second ECG, given that QRS complexes look almost the same as ECG n° 1.. Could it be initial transmural ischemia that transiently resolved but presented again later? Anyway, cath lab activation would have been unremarkable even on the basis of the first ECG alone.
Plus, in the third one, I personally wouldn't say "some inferior Q waves"; those look like inferior QS complexes (estabilished full-thickness inferior MI, possibly with resultant akinesis/scars on echocardiogram.
Thank BrooksWalsh, Dr. Smith and all of you guys!
By an Internal Medicine resident from italy and long-time follower of this blog
thank you Brooks. i don't even ever look a the computer interpretation like ever (Steve has told me that's not a great thing to do, to not look at all), well, sometimes , like if i have a question in my mind regarding blocks or rhythm, i'd look.
ReplyDeletethis is a clear OMI , i think, and i think there's a mm ST seg elevation in lead III if you use the T-P segment as Mattu suggests.
thank you, Brooks
tom