
Case submitted by Dr. Mike Runyon, written by Meyers, Grauer, and Smith
A child between the ages of 5 and 10 was brought in by parents for new onset recurrent episodes that were interpreted as most likely panic attacks. Before arriving at that diagnosis, the providers wanted to make sure all other diagnosable causes were ruled out. An ECG was ordered and is shown below.
 |
| What do you think? |
This was sent to me asking "What do you make of the T waves in V1 and V2?"
I responded:
"These T waves don't match any pathology I know of. I think they are likely just a meaningless normal variant. I've seen some like it before, and I've always failed to connect them with any pathology."
The ECG shows sinus rhythm with normal sinus P wave morphology, normal QRS axis and morphology for age, normal QT interval. There is a biphasic down-up T wave appearance in V1 and V2.
I sent it to Dr. Smith and Dr. Grauer who both agreed, and taught me that this is named "bifid T waves."
Below is a link to a study on bifid T waves
https://www.ncbi.nlm.nih.gov/
Study highlights:
- they define bifid T waves as those that are "notched, being the 2 peaks separate from each other by a notch with duration greater than or equal to 0.02 sec and voltage greater than or equal to 0.05 mV"
- they obtained an ECG on 604 consecutive children without known heart disease, then performed a "complete clinical and echocardiographic examination" on those with bifid T waves
- 110 children (18.3%) had bifid T waves, with the highest incidence in the 5 yr old age group
- bifid T waves were primarily detected in leads V2 and V3 (only 3.6% of cases found elsewhere)
- 110 consecutive healthy adults had no cases of bifid T waves
- No child with bifid T waves had a clinically significant abnormality found after clinical exam and echocardiogram
- QTc was normal in all subjects and did not differ between those with vs. without bifid T waves
- go to the link and see the very well done images and examples
Clinical Course
The patient had no medical cause of the episodes discovered, and was able to be safely discharged home with follow up.
Learning Points:
Bifid T waves appear to be a common finding in children between the ages of 3 and 10.
We believe they are likely a normal variant in this context, and the study above failed to identify any clinically significant finding after exam and echocardiogram in 110 children with bifid T waves.
Be careful to differentiate bifid T waves from other pathologic conditions such as hypokalemia (which can cause a U wave with prolonged QU interval) or non-conducted P waves hidden within the T wave.
===================================
MY Comment by KEN GRAUER, MD (7/10/2021):
===================================
Our appreciation to Dr. Runyon for this case. It is good to be aware of this normal variant in otherwise healthy children. I’d add the 3 following points to the discussion:
Point #1: When I first looked at leads V1 and V2 — I thought there may be 2 P waves for each QRS. Use of calipers quickly provided the answer (Figure-1).
- Note that the P-P interval is not the same between each of the P waves in lead V1. IF this was 2:1 AV block — then the P-P interval should be everywhere the same (with only occasional exception of some atrial tachycardias in adults that may not always be completely regular).
- The P-P interval between P waves “a-to-b” and “c-to-d” is the same (because P waves “b” and “d” are a part of the T wave, and are therefore related by a consistent distance to the previous QRS complex).
- Note that the P-P interval between P waves “b-to-c” and “d-to-e” are not the same! This is because the underlying rhythm of this young child is sinus arrhythmia — and this accounts for the variation (there would be no variation if this was 2:1 AV block).
- Looking in the limb leads (especially lead II, given the long R-R interval between the 2nd and 3rd beat in this lead) — We would expect to see an extra P wave if there was 2:1 block.
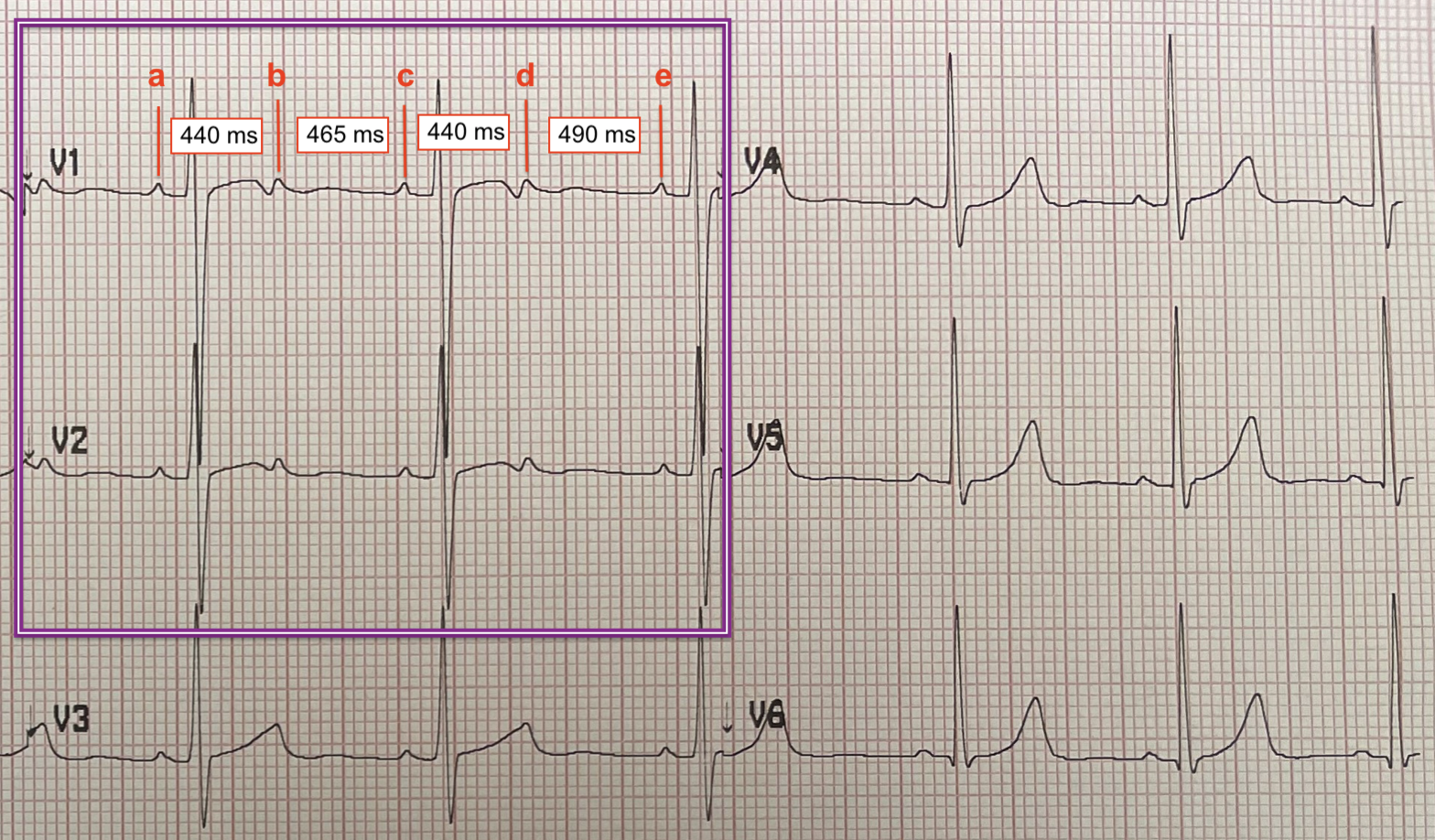 |
| Figure-1: Magnified view of the chest leads from today's tracing (See text). |
thxx
ReplyDeleteCame across this today and recognised instantly, thanks to this post.
ReplyDeleteSuper grateful for the work you all do here!