
This case was contributed by Brooks Walsh, an emergency physician in Connecticut.
The case
A middle aged patient had a convulsive episode while at work. EMS was called.
The convulsion ended by the time paramedics arrived, and the patient denied any symptoms.
The patient had a history of a severe nut allergy, and had eaten a snack soon before the convulsion. They were concerned the food may have had trace amounts of nuts in it, but there was no urticaria or wheezing.
During transport, however, the patient became sweaty and hypotensive. The paramedics were now concerned for anaphylaxis. Before administering IM epinephrine, the medic obtained an ECG:
The patient had a history of a severe nut allergy, and had eaten a snack soon before the convulsion. They were concerned the food may have had trace amounts of nuts in it, but there was no urticaria or wheezing.
During transport, however, the patient became sweaty and hypotensive. The paramedics were now concerned for anaphylaxis. Before administering IM epinephrine, the medic obtained an ECG:
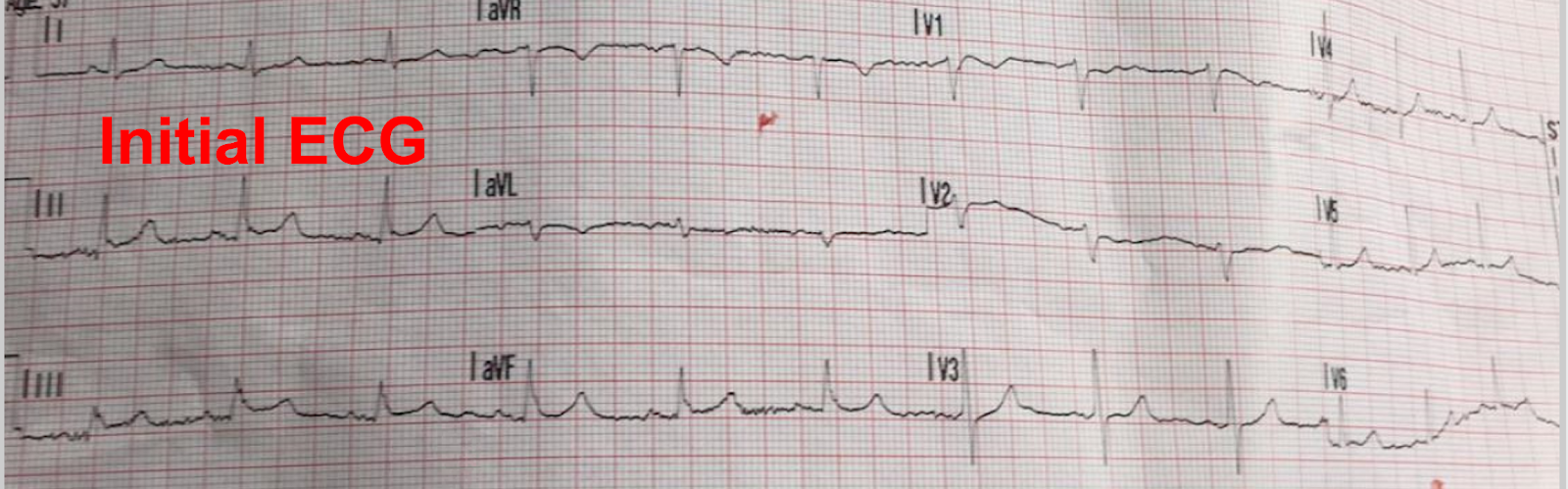 |
| There is some inferior ST Elevation, with probable notching at the J-point, which would be consistent with an early repolarization pattern. |
Epinephrine was given. The paramedic then noted a change in the monitoring lead about a minute later, and repeated the ECG:

ST elevation in the inferior leads and V5, V6
Reciprocal ST depression in leads I, aVL and V2.
Reciprocal ST depression in leads I, aVL and V2.
Diagnostic of acute occlusion MI.
So maybe that first one was not normal? Maybe it was the start of an inferior MI?
This was followed by an arrhythmia:
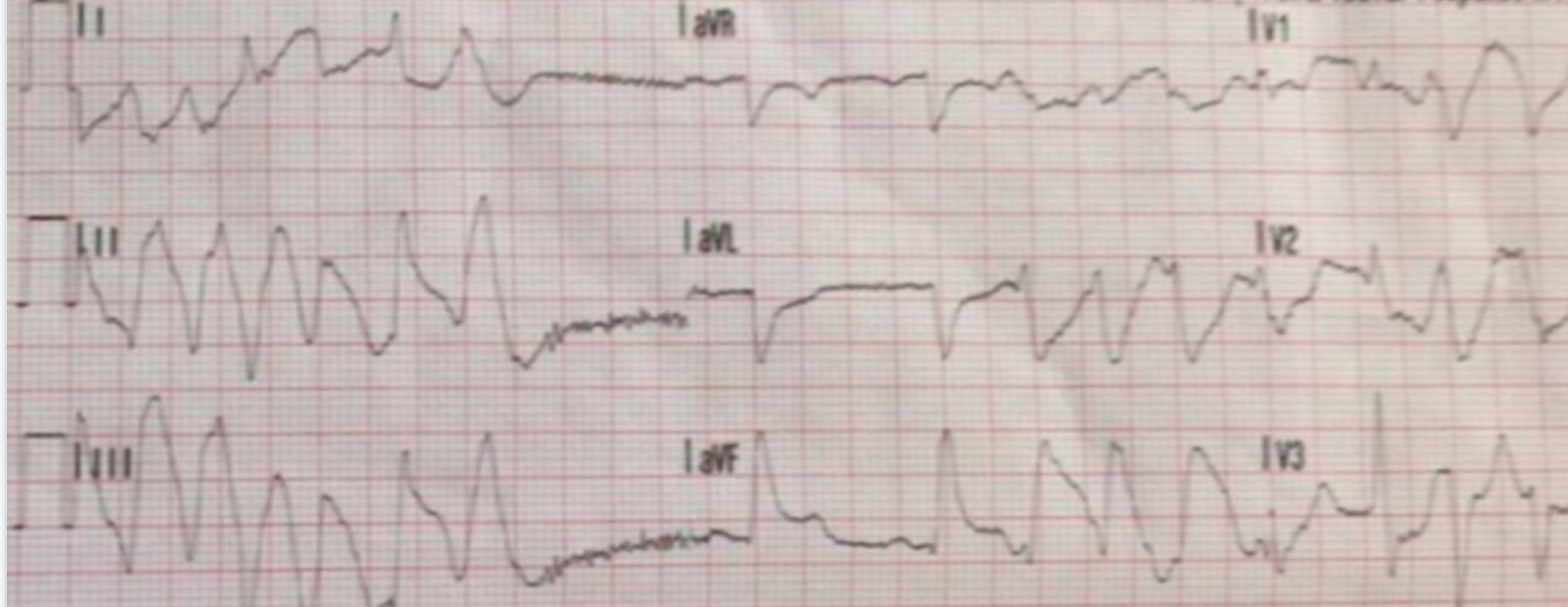
Polymorphic VT superimposed on persistent STE in aVF, STD in aVL.
The patient denied any chest pain or dyspnea despite these dramatic ECG changes . They appeared to be diaphoretic, but even this soon resolved.
The paramedic called for a cath lab activation. However, by the time they reached the ED, the ECG completely resolved:
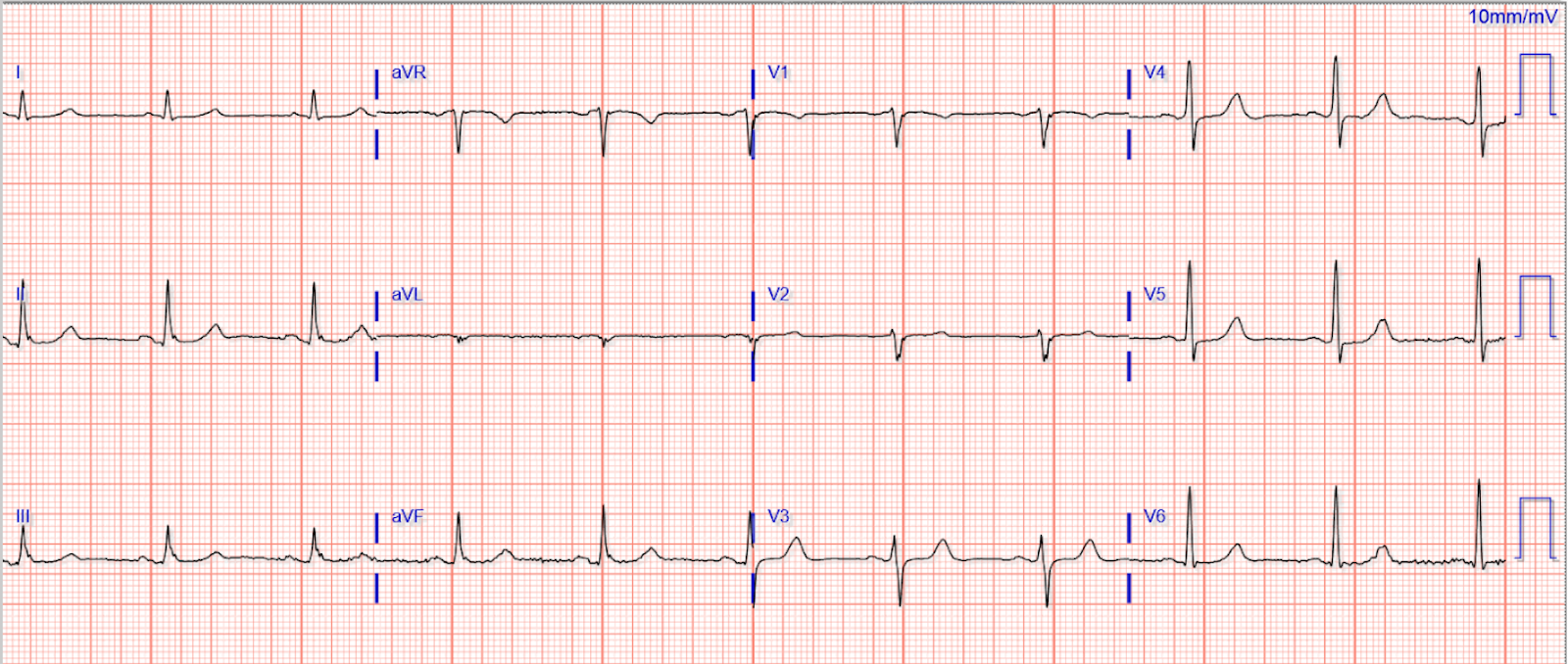
Completely normal
This could suggest that the subtle STE and reciprocal STD in the initial ECG were actually very early signs of MI
This could suggest that the subtle STE and reciprocal STD in the initial ECG were actually very early signs of MI
A hand-held echo (and subsequent comprehensive echo) did not reveal any wall-motion abnormalities, and the cath lab activation was cancelled. Serial troponins (non-hs) were undetectable. A subsequent exercise stress test was unremarkable.
So what could have caused the transient STEMI pattern?
I think the chief concern of many emergency clinicians is that IM epinephrine could provoke cardiac ischemia and an MI. There are several specific ways that epinephrine *might* have done this in this case:
If this had been a typical occlusion MI, though, the episode lasted for a significant amount of time, i.e. from the convulsion to the end of EMS transport. Despite that duration of time, there was no subsequent "bump" in troponin, no "stunned" myocardial wall motion but it should be pointed out that bedside ultrasound is EXTREMELY insensitive for wall motion abnormalities. With this EKG, it is impossible that there was NOT a wall motion abnormality. It was there but you did not see it. abnormalities seen, and no ECG evidence of spontaneous reperfusion (e.g. inferior TWI). One only sees such evolution in actual MI (as evidenced by troponin). With negative tropoinins, you do not expect any T-wave inversion. This is a case of unstable angina. The question is whether it is due to Epi, anaphylaxis, or to lysed thrombus.
So what could have caused the transient STEMI pattern?
I think the chief concern of many emergency clinicians is that IM epinephrine could provoke cardiac ischemia and an MI. There are several specific ways that epinephrine *might* have done this in this case:
- Demand ischemia can ischemia. But the second ECG shows a clearly localized area of ischemia, not typical of the global subendocardial ischemia (i.e. aVR ST elevation) that demand ischemia often produces.
- Epinephrine could have caused an isolated coronary vasospasm (e.g. of the RCA). This would produce a localized ischemia pattern, of course.
- Conversely, dilation of the other coronary vessels (from anaphylaxis), leading to relative stenosis of the RCA during stress (epinephrine) could produce localized ischemia by “coronary steal.” The exercise stress test, though, revealed no inducible ischemia, weighing against that possibility.
If this had been a typical occlusion MI, though, the episode lasted for a significant amount of time, i.e. from the convulsion to the end of EMS transport. Despite that duration of time, there was no subsequent "bump" in troponin, no "stunned" myocardial wall motion but it should be pointed out that bedside ultrasound is EXTREMELY insensitive for wall motion abnormalities. With this EKG, it is impossible that there was NOT a wall motion abnormality. It was there but you did not see it. abnormalities seen, and no ECG evidence of spontaneous reperfusion (e.g. inferior TWI). One only sees such evolution in actual MI (as evidenced by troponin). With negative tropoinins, you do not expect any T-wave inversion. This is a case of unstable angina. The question is whether it is due to Epi, anaphylaxis, or to lysed thrombus.
Can an appropriate dose of epinephrine for anaphylaxis cause an MI?
Unlikely!
Even if epinephrine was the cause of the STEMI pattern seen here, this would be rare. There are few such reported cases - this might only be the 8th in the literature. A recent review by Shrestha 2018 summarized prior cases:

Far more common than epinephrine-provoked MI is that the wrong dose or wrong route of epinephrine is administered. When the wrong dose is given by the wrong route, in particular, bad things can happen! The paramedic used an Epi-Pen in this case, making a dose ± route error practically impossible.
Here is another good reference: https://www.annemergmed.com/article/S0196-0644(17)30722-9/pdf
The only way to really rule out plaque rupture with thrombus that quickly lysed is to do intravascular coronary ultrasound to prove there is no ruptured plaque. It is very common for physicians to wrongly blame lysed thrombus on "spasm" without any objective evidence of spasm.
Take-away message: Properly administered epinephrine is extraordinarily unlikely to cause an MI.
Here is another good reference: https://www.annemergmed.com/article/S0196-0644(17)30722-9/pdf
The only way to really rule out plaque rupture with thrombus that quickly lysed is to do intravascular coronary ultrasound to prove there is no ruptured plaque. It is very common for physicians to wrongly blame lysed thrombus on "spasm" without any objective evidence of spasm.
Take-away message: Properly administered epinephrine is extraordinarily unlikely to cause an MI.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.