
This was texted to me, by a recent residency graduate, with the following information:
"70-something w hx of TAVR (aortic valve replacement) and Stroke. SVT w/aberrancy or VT?"
Here is what I texted back: "SVT. Give adenosine."
Response: "How did you tell?"
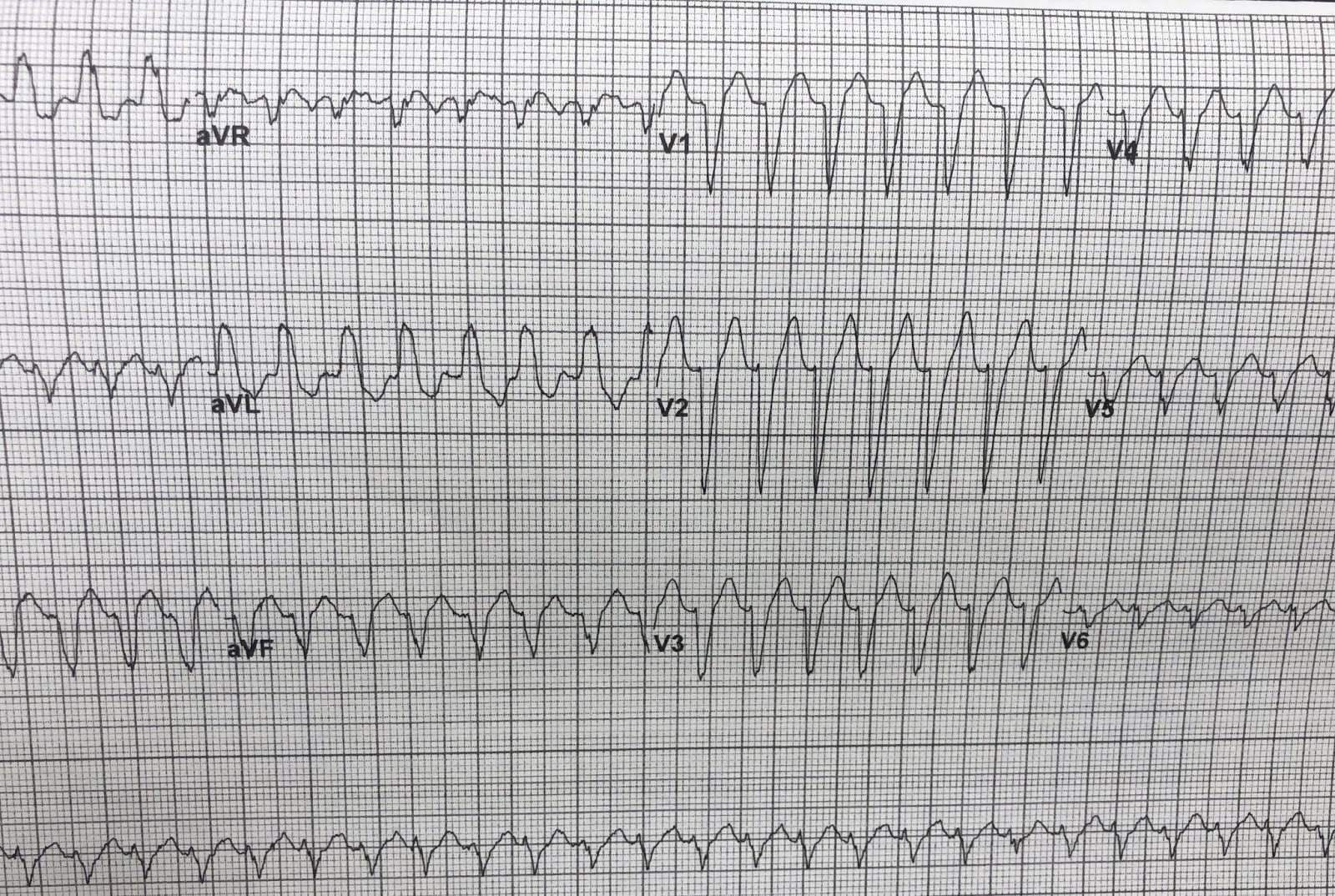
My answer: "Very rapid initial part of the QRS. Look at the right precordial leads: classic LBBB. aVR is negative and the initial deflection of the q-wave in aVR is only 20 ms"
I did not add: "except that the QRS in lateral leads V5 and V6 is negative. Although negative, there is a monophasic R-wave in the other lateral leads, I and aVL, typical of LBBB. The onset of the QRS in right precordial leads to the nadir of the S-wave is only about 40-50 ms. This is impossible in VT."
One is tempted to immediately conclude that this is VT because:
1. The patient is older with cardiac disease, which generally favors VT
2. One might be deceived into thinking there is concordance of the QRS in V1-V6 (all QRS in the same direction, which appears to be true). This is NOT TRUE however: concordance is NOT present. Concordance can only be called when the QRS is all one direction or all the other direction. If there is an RS-wave, then there cannot be concordance. Here, there are RS-waves in every precordial lead.
Answer: SVT with aberrancy. This was proven when a previous ECG in sinus was found and had the exact same LBBB morphology.
Explanation:
Typical VT (in contrast to fascicular VT) starts in myocardium, not in Purkinje fibers (conducting fibers). Therefore, the initial impulse takes some time to work its way through myocardium and therefore is traveling slowly (so it takes time and therefore many milliseconds to traverse). When it finally reaches conducting fibers, it then goes fast (narrow).
So in VT:
--The initial part of the QRS is slow [wide, with relatively small voltage change per change in time (or small Vi/Vt)], and the latter part of the QRS is fast (narrow, with relatively large Vi/Vt).
In SVT with aberrancy, the opposite is true:
The impulse is coming from above, from or through the AV node, and thus using conducting fibers. In SVT with aberrancy, there is some obstruction to the conduction such as RBBB or LBBB, but it is still able to go down some rapid pathway (the left bundle in RBBB or right bundle in LBBB) and only LATER must go through myocardium to arrive at the remainder of the heart.
Thus:
--The initial part of the QRS is fast (narrow, with relatively large Vi/Vt), and the latter part of the QRS is slow (wide, with relatively small Vi/Vt).
Another good rule:
If it looks exactly like LBBB or RBBB, then it is SVT with aberrancy. But beware: if it looks like LBBB but has a wide r-wave in V1, then it is VT. If it looks like RBBB, but has a wide r-wave in V1, then is is probably VT.
Finally, strictly speaking, this is not "aberrancy" because there was pre-existing BBB; aberrancy implies that the LBBB or RBBB is a result of the tachycardia, not a baseline finding. But of course until you find that old ECG, you will not know. So that is of academic significance.
Management:
Of course either VT or SVT with aberrancy can be treated with electrical cardioversion, but unless the patient is in severe shock or pulmonary edema, you have time to give adenosine. If it is VT, adenosine is safe. Adenosine is NOT safe if the rhythm is irregular and polymorphic, implying possible Atrial fibrillation with WPW.
Jerry Jones added these useful comments:
Regarding the negative QRS complex in V6: you see this a lot with left bundle branch block. The impulse has to enter the LV transseptally from the RV. In so doing, the impulse may enter the posterior fascicle first, since it lies right next to the septum. While this is not generally considered LAFB, you get the same effect because the posterior fascicle is activated first, followed by the anterior fascicle. This is also what is causing the marked left axis deviation.
The R-to-S nadir value is also very helpful, though a fascicular VT could also present that way. However, the width of these QRS complexes would be rather wide for a fascicular complex. Some of the upslope of the "T" wave in the precordial leads is actually QRS. You can see this by measuring the QRS width in a few of the limb leads with your calipers and then comparing the width of the QRS in the precordial leads.


"70-something w hx of TAVR (aortic valve replacement) and Stroke. SVT w/aberrancy or VT?"
 |
| What do you think? |
Here is what I texted back: "SVT. Give adenosine."
Response: "How did you tell?"
My answer: "Very rapid initial part of the QRS. Look at the right precordial leads: classic LBBB. aVR is negative and the initial deflection of the q-wave in aVR is only 20 ms"
I did not add: "except that the QRS in lateral leads V5 and V6 is negative. Although negative, there is a monophasic R-wave in the other lateral leads, I and aVL, typical of LBBB. The onset of the QRS in right precordial leads to the nadir of the S-wave is only about 40-50 ms. This is impossible in VT."
One is tempted to immediately conclude that this is VT because:
1. The patient is older with cardiac disease, which generally favors VT
2. One might be deceived into thinking there is concordance of the QRS in V1-V6 (all QRS in the same direction, which appears to be true). This is NOT TRUE however: concordance is NOT present. Concordance can only be called when the QRS is all one direction or all the other direction. If there is an RS-wave, then there cannot be concordance. Here, there are RS-waves in every precordial lead.
Answer: SVT with aberrancy. This was proven when a previous ECG in sinus was found and had the exact same LBBB morphology.
Explanation:
Typical VT (in contrast to fascicular VT) starts in myocardium, not in Purkinje fibers (conducting fibers). Therefore, the initial impulse takes some time to work its way through myocardium and therefore is traveling slowly (so it takes time and therefore many milliseconds to traverse). When it finally reaches conducting fibers, it then goes fast (narrow).
So in VT:
--The initial part of the QRS is slow [wide, with relatively small voltage change per change in time (or small Vi/Vt)], and the latter part of the QRS is fast (narrow, with relatively large Vi/Vt).
In SVT with aberrancy, the opposite is true:
The impulse is coming from above, from or through the AV node, and thus using conducting fibers. In SVT with aberrancy, there is some obstruction to the conduction such as RBBB or LBBB, but it is still able to go down some rapid pathway (the left bundle in RBBB or right bundle in LBBB) and only LATER must go through myocardium to arrive at the remainder of the heart.
Thus:
--The initial part of the QRS is fast (narrow, with relatively large Vi/Vt), and the latter part of the QRS is slow (wide, with relatively small Vi/Vt).
Another good rule:
If it looks exactly like LBBB or RBBB, then it is SVT with aberrancy. But beware: if it looks like LBBB but has a wide r-wave in V1, then it is VT. If it looks like RBBB, but has a wide r-wave in V1, then is is probably VT.
Finally, strictly speaking, this is not "aberrancy" because there was pre-existing BBB; aberrancy implies that the LBBB or RBBB is a result of the tachycardia, not a baseline finding. But of course until you find that old ECG, you will not know. So that is of academic significance.
Management:
Of course either VT or SVT with aberrancy can be treated with electrical cardioversion, but unless the patient is in severe shock or pulmonary edema, you have time to give adenosine. If it is VT, adenosine is safe. Adenosine is NOT safe if the rhythm is irregular and polymorphic, implying possible Atrial fibrillation with WPW.
Jerry Jones added these useful comments:
Regarding the negative QRS complex in V6: you see this a lot with left bundle branch block. The impulse has to enter the LV transseptally from the RV. In so doing, the impulse may enter the posterior fascicle first, since it lies right next to the septum. While this is not generally considered LAFB, you get the same effect because the posterior fascicle is activated first, followed by the anterior fascicle. This is also what is causing the marked left axis deviation.
The R-to-S nadir value is also very helpful, though a fascicular VT could also present that way. However, the width of these QRS complexes would be rather wide for a fascicular complex. Some of the upslope of the "T" wave in the precordial leads is actually QRS. You can see this by measuring the QRS width in a few of the limb leads with your calipers and then comparing the width of the QRS in the precordial leads.
-----------------------------------------------------------
Comment by KEN GRAUER, MD (1/28/2019):
-----------------------------------------------------------
Great example by Dr. Smith of the common emergency medicine dilemma of the “regular WCT”. While my thoughts on management of this case are similar to those by Dr. Smith = Assuming this patient is hemodynamically stable, begin with a diagnostic/therapeutic trial of Adenosine — I will offer a few differing thoughts on my decision-making approach. This subject remains one that invites active discussion — and this is the goal of my comments below.
- For clarity — I reproduce and label the ECG in this case in Figure-1.
 |
| Figure-1:The initial ECG in this case (See text). |
==========================
I always start by description of what we have — which in this case is a regular WCT (= Wide-Complex Tachycardia) at ~170/minute without clear sign of atrial activity. We need confirmation that this patient is hemodynamically stable — because if not, then regardless of whether the rhythm is VT or SVT (with either preexisting BBB or aberrant conduction) — immediate synchronized cardioversion would be indicated.
- The literature suggests that statistically — the etiology of a regular WCT without clear sign of atrial activity will turn out to be VT in at least 80% of cases. If the patient is “older” and has underlying heart disease (as is the case for this patient) — statistical likelihood of VT before you even look at the ECG goes up to ~90%. I’ll emphasize that 90% is not 100% — and this case provides the perfect example of when ECG characteristics substantially reduce statistical likelihood of VT — but: i) I think it helpful to be aware of this information regarding statistical likelihood; ii) As a result of this statistical likelihood, we need to consider VT until proven otherwise; iii) Even if the rhythm is VT — IF the patient is hemodynamically stable — you do not necessarily have to immediately shock VT. Instead, additional diagnostic measures while you try to increase your diagnostic certainty (including potential diagnostic/therapeutic trial with an agent such as Adenosine) is perfectly reasonable.
- Rather than distinguishing between only 2 diagnostic entities ( = VT vs SVT, with either preexisting BBB, SVT with aberration, or AVRT with anterograde conduction over an accessory pathway) — I am in favor of considering 3 Diagnostic Entities: i) definite VT; ii) definite SVT; or, iii) being unable to attain >95-100% certainty in distinguishing between VT or SVT. I view this particular case ( = my opinion) as iii = being unable to attain >95-100% certainty of the rhythm diagnosis from the single tracing shown in Figure-1.
- KEY POINT: You will often not be able to attain >95-100% certainty about the diagnosis of a regular WCT rhythm at the time you need to begin treatment. I’m happy to acknowledge the clinical reality of this diagnostic uncertainty.
The literature is replete with criteria for distinguishing between VT vs SVT with either preexisting BBB or aberrant conduction. Each set of criteria has its set of advocates. I reference some of my sources below, and summarize my approach HERE. Two criteria that approach 100% specificity for VT are: i) Global concordance in the chest leads (ie, all 6 chest leads show either all positive or all negative QRS complexes); and, ii) AV dissociation.
- Although the QRS complex is almost all negative in all 6 chest leads in Figure-1 — it most definitely is not all negative (RED circles highlight a small-and-thin initial r wave in leads V2-thru-V5). This criterion of global concordance of chest leads is only helpful if ALL 6 chest leads are completely positive or completely negative. If even one chest lead shows both an r and s wave — the diagnostic specificity of this criteria is completely negated. Practically speaking — it will be rare (<10% of WCT rhythms) that you see global concordance (either positive or negative concordance) in all 6 chest leads — so most of the time this criterion will not be helpful. Therefore, great if you see it — but not helpful if you don’t.
- Note that in Figure-1, the initial positive deflection in lead V6 is actually WIDE, as well as notched (BLUE arrow). If anything — this morphologic feature is a factor in favor of VT.
- It’s wonderful when you can reliably identify AV dissociation within a regular WCT — because this finding would then be diagnostic of VT. That said, in my experience — the phenomenon of AV dissociation is greatly overused, and overdiagnosed. One needs to see clear evidence of an underlying regular atrial rhythm that is completely unrelated to ventricular complexes. Despite variation in T wave morphology throughout the long lead II rhythm strip in Figure-1 (that I suspect may represent some form of atrial activity) — I’m unable to confirm (with calipers) a consistent independent underlying atrial rhythm. Therefore, the criterion of AV dissociation cannot be used here.
- Beyond-the-Core: Unfortunately, the tracing in Figure-1 is markedly distorted by changing angulation of the grid lines. This prevents me from exploring what seems to be slight-but-definite repetitive variation in the R-R interval (long-short) during parts of the tracing. There may indeed be hidden atrial activity … but I'd need a better quality tracing to explore this. In any event, I see no proof of AV dissociation.
Consistent delay in the initial QRS deflection (or in the time until one attains the R-to-S nadir in any precordial lead) — is clearly a helpful criterion that favors VT. The problem (to my reading of the literature) — is that lack of such delay is not definitive for ruling out VT. So while the limb leads in Figure-1 certainly look typical of a supraventricular LBBB pattern, and the predominantly negative QRS complexes in V1, V2, V3 with tiny thin r waves could be consistent with LBBB — the less than-vertical descent of these anterior S waves (thin RED lines suggesting r-to-s nadir ~0.04-0.05 second) and, lack of monophasic R wave in lead V6 with wide-and-notched-but-small initial r wave in this V6 lead are morphologic features that are not expected with typical LBBB. I do not think ( = my opinion) QRS morphology in Figure-1 is definitive for LBBB.
- CAVEAT #1: Some patients have decidedly atypical baseline BBB patterns due to scarring from prior infarction and/or cardiomyopathy. Finding a prior ECG on the patient may prove invaluable in such cases (as it did here) — by confirming that the atypical QRS morphology during the WCT is identical to the patient’s baseline QRS pattern. That said, most of the time you will unfortunately not have access to a prior ECG at the moment you need to begin management.
- CAVEAT #2: In my experience, the presence of extreme axis deviation (in which the QRS complex is entirely negative in either lead I or in lead aVF) — is very helpful in suggesting that a regular WCT rhythm is VT. That said, patients with LBBB may sometimes manifest an entirely negative QRS complex in lead aVF ...
- CAVEAT #3: While QRS morphology with “typical” LBBB should manifest a monophasic R wave in both left-sided leads I and V6 — some patients do not show a monophasic R wave in the chest leads until you reach a V7 or V8 lateral position. This is especially true in patients with marked LVH, in which the predominant vector of LV depolarization is directed not only laterally, but also to a great extent posteriorly.
BOTTOM LINE — My initial impression of the regular WCT rhythm in Figure-1 was that despite some atypical features — parts of the tracing clearly suggest a supraventricular LBBB pattern. When the patient in front of you is hemodynamically stable — this is the ideal situation for a diagnostic/therapeutic trial of Adenosine. It is also the ideal situation to assign an “extra hand” at the bedside to quickly search the chart for a prior ECG — that in this case enabled definitive determination that the rhythm in Figure-1 was indeed SVT with preexisting BBB, and not VT.
==========================
==========================
Selected References:
- Brugada P, Brugada J, Mont L, et al: A New Approach to the Differential Diagnosis of a Regular Tachycardia with a Wide QRS Complex. Circulation 83:1649-1659, 1991.
- Blomstrom-Lundqvist C, Scheinman MM, Aliot EM, et al: ACC/AHA/ESC Guidelines for Management of Patients with Supraventricular Arrhythmias — Executive Summary. J Am Coll Cardiol 42:1493-1531, 2003.
- Vereckei A, Duray G, Szenasi G: Application of a New Algorithm in the Differential Diagnosis of Wide QRS Complex Tachycardia. Eur Heart J 28:589-600, 2007.
- Sasaki K: A New Simple Algorithm for Diagnosing Wide QRS Complex Tachycardia: Comparison with Brugada, Vereckei and aVR Algorithms. Circulation 120:S671, 2009.
- Click HERE — for My Approach to the Regular WCT.
Great explanation
ReplyDeleteSteve...
ReplyDeleteThis is a great teaching ECG! I'm very glad to see your comments on concordance in the precordial leads. I have seen authors state that the QRS complexes only have to be "mostly" positive or "mostly" negative and I even saw one article where the author stated that only "most of the precordial leads" had to have the same orientation! Where did this start to go so wrong?
Regarding the negative QRS complex in V6: you see this a lot with left bundle branch block. The impulse has to enter the LV transseptally from the RV. In so doing, the impulse may enter the posterior fascicle first, since it lies right next to the septum. While this is not generally considered LAFB, you get the same effect because the posterior fascicle is activated first, followed by the anterior fascicle. This is also what is causing the marked left axis deviation.
The R-to-S nadir value is also very helpful, though a fascicular VT could also present that way. However, the width of these QRS complexes would be rather wide for a fascicular complex. Some of the upslope of the "T" wave in the precordial leads is actually QRS. You can see this by measuring the QRS width in a few of the limb leads with your calipers and then comparing the width of the QRS in the precordial leads.
Jerry,
DeleteGreat comments. Thanks.
Fascicular VT acts a lot like SVT anyway because it does not have the associated low EF.
We have an entire article on fascicular VT.
http://hqmeded-ecg.blogspot.com/2018/09/idiopathic-ventricular-tachycardias-for.html
Steve
why they're called RS in precordial lead? aren't they rS?
ReplyDeleteYes, but whether RS or rS or Rs, one cannot call concordance.
DeleteVT vs SVT: often the explanations are complicated and
ReplyDeletenot always understandable; your explanations are simple
and go to the point.(Myocardium vs Fibers)
Merci et félicitations
Al
Al,
DeleteMerci a vous!
Steve
Thank you very much, I've to study this.
ReplyDeleteI've found a very hepful publication 10.15420/aer.2013.2.1.23
Regards from Chile!
Awesome!
ReplyDeleteGreat and helpful explaination
ReplyDelete