
A young woman presented with status seizures and apparent overdose of bupropion. There was a question of cocaine use too (with later suspicion of possible ingestion or body stuffing).
She had status seizures for which she was intubated and medically treated (successfully) with propofol and benzos.
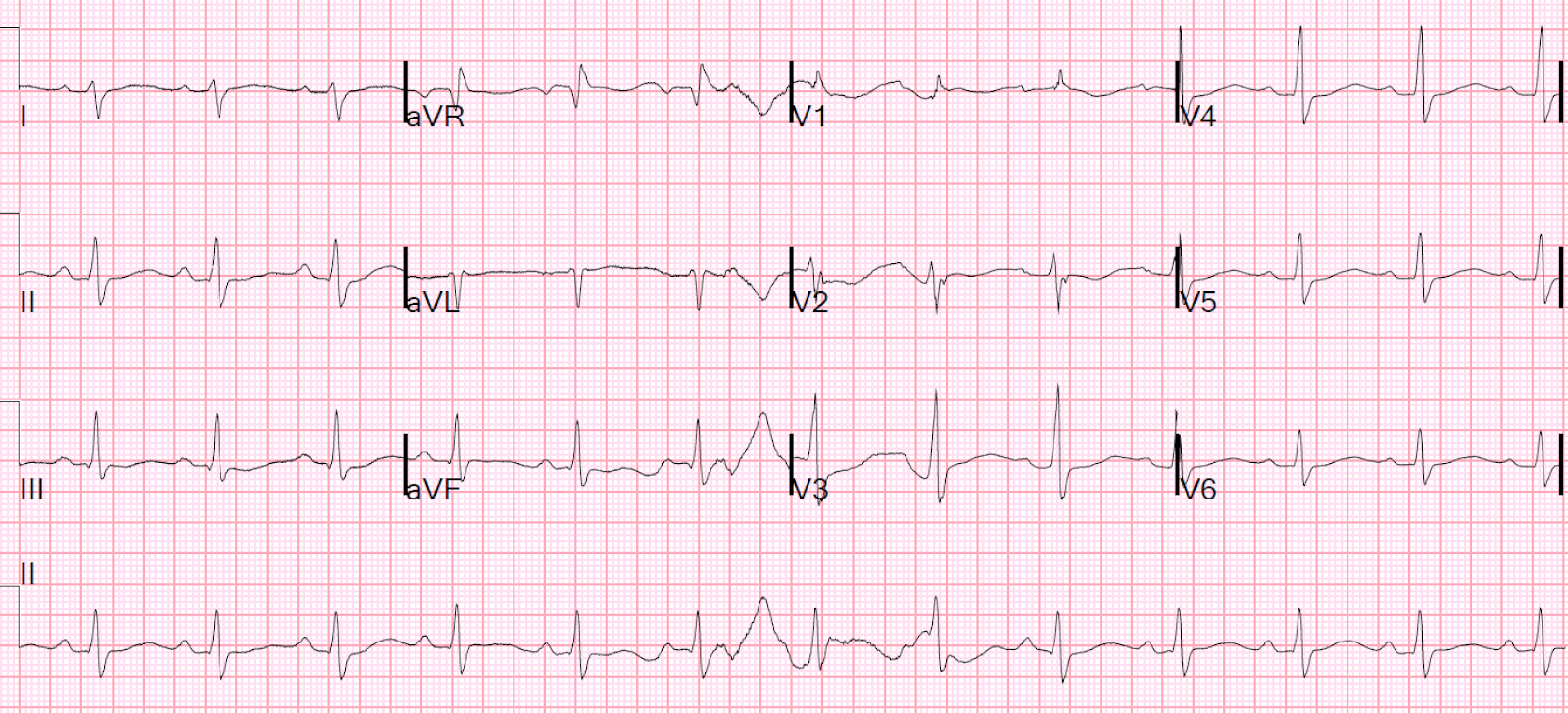
An ECG was recorded:
This was recorded 8 hours later:
Shortly thereafter, the patient had a witnessed PEA arrest that resolved with epinephrine and bicarbonate.
The arrest was not due to an arrhythmia (not Torsades de Pointes).
Here is the post arrest ECG:
The exact etiology of the PEA arrest was uncertain but a because the Na channel blocking activity, sodium bicarb was given and the patient stabilized. (Most arrest from wide QRS in Na channel blockade starts with ventricular tachycardia, and most with long QT starts with polymorphic VT (Torsades de Pointes).)
The next day, this was recorded at a time when electrolytes were normal:
Troponin returned at 4.5 ng/mL.
The tox consultant texted me to confirm her opinion that this is not STEMI. Is it?
Is it STEMI? No. There is a bizarrely long QT interval. My measurement = 520 ms (Bazett correction = 634 ms; Fridericia correction 591 ms).
The morphology of the ST segment is just not right for STEMI.
Moreover, the clinical context is not right for STEMI. It is right for acute myocardial injury due to direct toxic effect or to type 2 myocardial infarction due to hypoperfusion during arrest or shock.
This is an ECG that one would commonly see in Takotsubo Stress Cardiomyopathy, whether or not there is actual echo evidence of it.
No echo was done, but my advice was that this was a purely toxicologic ECG, with extremely long QT.
EKG day 3:
EKG day 4:

The patient eventually did well and recovered.
Learning Points:
1. Recognize the effects of sodium channel blockade: large R-wave in aVR and widened QRS, often with RBBB morphology.
2. A widened QRS in Na channel blockade toxicity is very dangerous and often leads to cardiac arrest
3. The computer is terrible at measuring the QT interval. You must measure it yourself.
4. Not all acute ST elevation is due to acute coronary occlusion.
5. A large bupropion overdose can be very dangerous


She had status seizures for which she was intubated and medically treated (successfully) with propofol and benzos.
An ECG was recorded:
 |
| Sinus tach, with a slightly widened QRS (113 ms) and slightly long QT There is a slightly abnormally large R-wave in aVR. So there might be some sodium channel blockade here, which is expected with cocaine. Bicarbonate was given. |
This was recorded 8 hours later:
 |
| QRS = 148 ms and large R-wave in aVR (very dangerous) This is typical of Na channel blockade. Bupropion and Cocaine are both powerful Na channel blockers. Computerized QTc = 486 ms Bazett correction = 546 ms Fridericia correction = 528 ms My measurement = 550 ms Bazett = 618 ms Fridericia = 598 ms (Very long QT) |
Shortly thereafter, the patient had a witnessed PEA arrest that resolved with epinephrine and bicarbonate.
The arrest was not due to an arrhythmia (not Torsades de Pointes).
Here is the post arrest ECG:
 |
| There is RBBB with QRS duration is 137 ms and there is a very large R-wave in aVR. There are 2 bumps on the T-wave; one could be a U-wave. Since a long QU is also dangerous, let's assume it is all T-wave. Computerized QT = 420 ms, with QTc = 490 ms. I measure 480 ms. Fridericia correction = 615 ms. Very long. |
The exact etiology of the PEA arrest was uncertain but a because the Na channel blocking activity, sodium bicarb was given and the patient stabilized. (Most arrest from wide QRS in Na channel blockade starts with ventricular tachycardia, and most with long QT starts with polymorphic VT (Torsades de Pointes).)
The next day, this was recorded at a time when electrolytes were normal:
 |
| There is ST elevation and large T-waves. The computer read ***STEMI*** It does meet STEMI criteria of at least 1.5 mm in V2 and V3 in a woman. Is this STEMI? Computerized QT = 462 (Bazett correction = 556 ms; Fridericia correction = 525 ms) |
The tox consultant texted me to confirm her opinion that this is not STEMI. Is it?
Is it STEMI? No. There is a bizarrely long QT interval. My measurement = 520 ms (Bazett correction = 634 ms; Fridericia correction 591 ms).
The morphology of the ST segment is just not right for STEMI.
Moreover, the clinical context is not right for STEMI. It is right for acute myocardial injury due to direct toxic effect or to type 2 myocardial infarction due to hypoperfusion during arrest or shock.
This is an ECG that one would commonly see in Takotsubo Stress Cardiomyopathy, whether or not there is actual echo evidence of it.
No echo was done, but my advice was that this was a purely toxicologic ECG, with extremely long QT.
EKG day 3:
 |
| QRS 110 Computerized QT 415, QTc 441 Again, there is an extremely long QT that the computer did not detect.Large U-waves, K = 3.9 |
EKG day 4:

The patient eventually did well and recovered.
Learning Points:
1. Recognize the effects of sodium channel blockade: large R-wave in aVR and widened QRS, often with RBBB morphology.
2. A widened QRS in Na channel blockade toxicity is very dangerous and often leads to cardiac arrest
3. The computer is terrible at measuring the QT interval. You must measure it yourself.
4. Not all acute ST elevation is due to acute coronary occlusion.
5. A large bupropion overdose can be very dangerous
-----------------------------------------------------------
Comment by KEN GRAUER, MD (7/20/2018):
-----------------------------------------------------------
Superb case by Dr. Smith for illustrating sequential effects of Sodium-Channel Blockade with the important clinical implications to be aware of. I’d add the following:
- Great example of how serial ECGs on this patient simulate a number of other ECG conditions. As per Dr. Smith — despite troponin elevation and ST elevation in leads V2 and V3 of the 4th ECG — both the shape of these ST segments and the clinical context argued strongly against this being a STEMI.
- Similarly, despite the QRS widening, upright R wave in V1 and S waves in lateral leads in the first 3 ECGs — the shape of the QRS in lead V1 was not suggestive of RBBB due to a conduction defect. For a QRS complex as wide as it is in these tracings — one simply would not expect the small (less than 5mm tall) amount of R wave positivity and narrowness that we see in V1 if there was true RBBB. Instead, the clinical context + combination of marked right axis, large terminal R wave in aVR plus QRS prolongation with marked QTc widening suggests severe toxic overdose as the cause of these ECG abnormalities (Figure-1).
- The KEY to optimal use of computerized interpretations lies with knowing HOW to use the computer. Computers analyze data. If data-IN is poor — then data-OUT will be poor. The ECGs in this case for which computer estimation of the QTc was grossly inaccurate, showed baseline artifact + indistinct borders for the end of the QT interval in most leads. If YOU are having trouble quickly discerning where the QT interval ends — then the computer will also have trouble doing so. In such cases — Do NOT expect computer estimation of the QTc to be at all accurate. In contrast — when artifact is minimal or absent, and the onset and offset of the QT interval is easy to ascertain on the ECG — it is much more likely that the computer WILL be accurate in its assessment of intervals. This does NOT mean that you should ever accept computer values without overreading them. But it does mean that no more than a brief glance may be needed for you to validate that the computer is accurate in its assessment of intervals when the quality of the tracing is good, and all limits are clearly definable. That said, in THIS case — it should be obvious from the start that the computer can not be trusted at all for its assessment of any interval.
- To clarify the process of QTc estimation in this case — I’ve marked in Figure-1 the 2 leads in which I am comfortable with my notation of where I believe the QT interval ends. I measure the QT ~550-560ms — which at a heart rate of ~75/minute, corrects to a QTc of >600ms! We could also have used lead V4 to assess the QT in this tracing — but probably none of the other 9 leads. The indistinct delineation of the end of the QT interval explains how the computer estimate of 486ms for the QTc came to be so far off from what the QTc actually is.
 |
| Figure-1: 2nd ECG in this case — illustrating atypical RBBB morphology and indistinct borders for the end of the QTc in most leads. (See text). |
Our THANKS to Dr. Smith for this rare insight into the serial ECG changes of severe Sodium-Channel Blockade!
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.