
A middle-aged male with h/o CABG x 3, previous stents, and aortic valve and aortic root replacement presented primarily with headache, but also told the medics that he had chest pain (for 6 hours) because he "knew they would respond faster than if he said headaches." The chest pain was right sided rib and shoulder pain, worse with inspiration, sharp, and sometimes 7-8/10. But the headache was much worse. Chest pain was not relieved by sublingual NTG.
He has noticed worsening exertional dyspnea, such that he feels he can only walk about a block before experiencing "chest tightness.
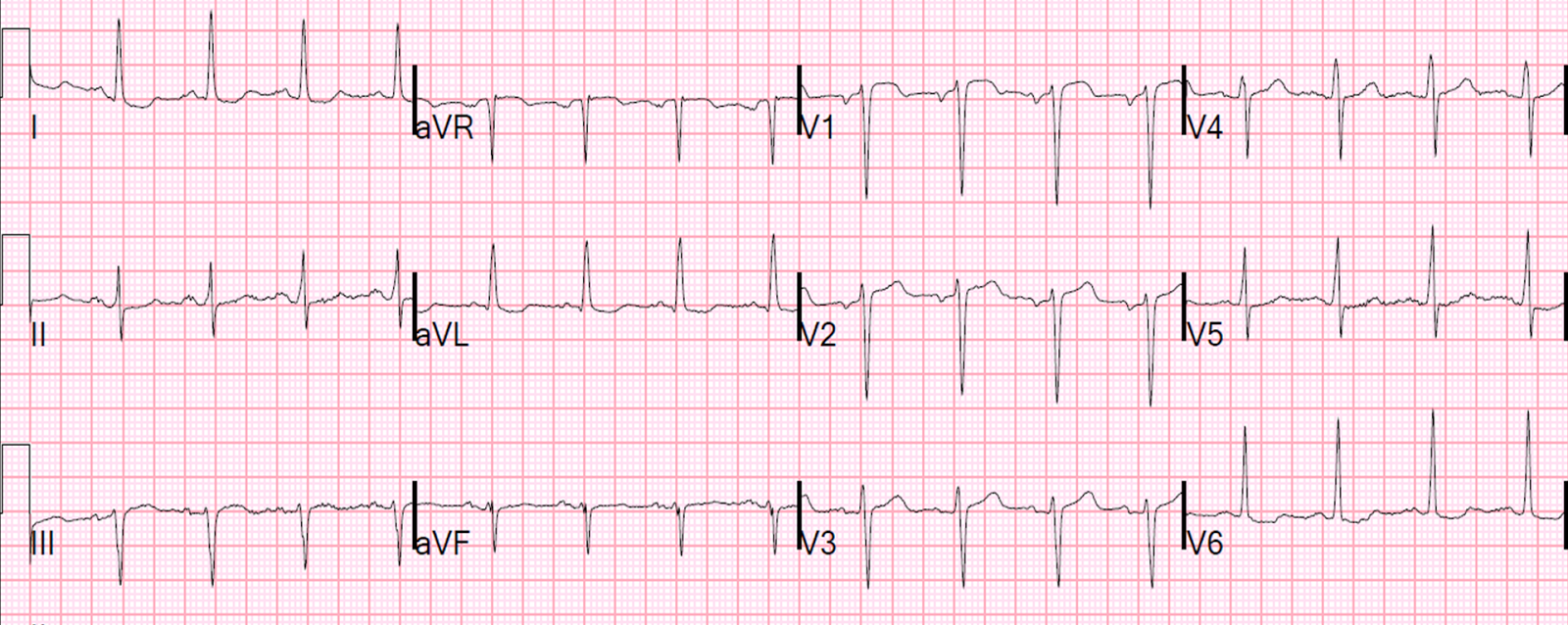
Here is his ED ECG (compare with the 2 month previous ECG below it):
Previous ECG from 2 months prior:
CT head was negative for acute bleed. The patient was managed medically with ASA 325 mg, heparin, and Plavix, and nitroglycerine, but his pain did not improve. A troponin I returned at 7.7 ng/mL (diagnostic of MI).
A repeat ECG was recorded:
Cardiology was consulted for NSTEMI that needs the cath lab now (objective evidence of ischemia and ongoing pain). The cath lab was activated.
Cath results:
I ran across this case and this ECG while reading through a series of ECGs and it alarmed me. The inferior ST elevation is now gone, but there is new DIAGNOSTIC ST elevation in V1-V3. Look closely: the ST elevation is greatest in V1 and V2, and does not extend out to V4.
Why? Because this "anterior" MI is due to STEMI of the right ventricle (RV), not of the LV.
Case Progression
The cardiologist quickly went to evaluate the patient, who found that the chest pain was unchanged and that the patient was hemodynamically stable. A formal echo showed some RV dysfunction and normal LV anterior wall.
This was presumed to be an isolated acute RV infarction and due to the patient stability and the difficulty of the coronary anatomy, no intervention was undertaken. Presumably, the procedure induced a thrombus in the RV marginal branch.
This was recorded 3 hours post cath:
5 hours post cath:
Next day:

The troponin I peaked at 29, fell to 20, then rose again just a little to 21.5 ng/mL due to the brief RV STEMI.
The patient did well.
Learning points:
1. NonSTEMI often need immediate cath lab activation. as I have often discussed.
2. STEMI in V1-V3 is anterior, but not necessarily due to LV anterior STEMI. It may be due to RV STEMI, which is also anterior.
3. When the RCA is the vessel involved, new anterior ST elevation is likely to be RV STEMI
4. When the ST elevation is greatest in V1-V3 vs. V2-V4, RV STEMI is more likely than LV
Detailed cath results:
He has noticed worsening exertional dyspnea, such that he feels he can only walk about a block before experiencing "chest tightness.
Here is his ED ECG (compare with the 2 month previous ECG below it):
 |
--Is there a new Q-wave (tiny r-wave) in III?
--There is new ST elevation in III, with new STE also in aVF.
--There is reciprocal ST depression in aVL.
--There is STE in V1, suggesting RV MI, but this was present on the old one.
--There is some ST depression in V5 and V6.
--This is almost certainly an acute inferior MI, though does not meet mm "criteria" for STEMI
--The beginnings of T-wave inversion suggest an open artery.
|
Previous ECG from 2 months prior:
 |
| Previous, does not have the same ST deviations |
CT head was negative for acute bleed. The patient was managed medically with ASA 325 mg, heparin, and Plavix, and nitroglycerine, but his pain did not improve. A troponin I returned at 7.7 ng/mL (diagnostic of MI).
A repeat ECG was recorded:
 |
| There is slightly more STE in III and reciprocal STD in aVL |
Cardiology was consulted for NSTEMI that needs the cath lab now (objective evidence of ischemia and ongoing pain). The cath lab was activated.
Cath results:
It was a complex cath and anatomy. The RCA was diffusely diseased and had an acute on chronic occlusion that was opened.
A Post Cath ECG was obtained an hour later:
 |
| What is going on? |
I ran across this case and this ECG while reading through a series of ECGs and it alarmed me. The inferior ST elevation is now gone, but there is new DIAGNOSTIC ST elevation in V1-V3. Look closely: the ST elevation is greatest in V1 and V2, and does not extend out to V4.
Why? Because this "anterior" MI is due to STEMI of the right ventricle (RV), not of the LV.
Case Progression
The cardiologist quickly went to evaluate the patient, who found that the chest pain was unchanged and that the patient was hemodynamically stable. A formal echo showed some RV dysfunction and normal LV anterior wall.
This was presumed to be an isolated acute RV infarction and due to the patient stability and the difficulty of the coronary anatomy, no intervention was undertaken. Presumably, the procedure induced a thrombus in the RV marginal branch.
This was recorded 3 hours post cath:
 |
| The RV infarct appears to be resolving spontaneously. |
5 hours post cath:
 |
| More resolution of ST elevation, with some T-wave inversion. This is good evidence of spontaneous reperfusion of the RV marginal branch |
Next day:

The troponin I peaked at 29, fell to 20, then rose again just a little to 21.5 ng/mL due to the brief RV STEMI.
The patient did well.
Learning points:
1. NonSTEMI often need immediate cath lab activation. as I have often discussed.
2. STEMI in V1-V3 is anterior, but not necessarily due to LV anterior STEMI. It may be due to RV STEMI, which is also anterior.
3. When the RCA is the vessel involved, new anterior ST elevation is likely to be RV STEMI
4. When the ST elevation is greatest in V1-V3 vs. V2-V4, RV STEMI is more likely than LV
Detailed cath results:
1) 2 vessel CABG [Left internal mammary (LIMA) to LAD, and Saphenous Vein Graft (SVG) to left posterolateral artery (L-PLA)]
months ago.
3) The SVG to the L-PLA is occluded. The LIMA to the Mid-LAD is widely
patient.
4) The RCA was patent on the cath of xxxxxxx. The occluded RCA currently
likely represents acute on chronic obstruction in light of the patients
clinical presentation and the collaterals to the R-PDA.
5) Balloon angioplasty only due to noncompliance with clopidogrel,
reducing the sub-total occlusion to diffuse 30-40% stenosis. The R-PDA is
occluded proximally and was probe with a wire.
Coronary Angiograms
LMCA: 60% calcified mid to distal LM stenosis.
LAD: Multiple stents in the LAD system. Sub-totally occluded LAD after the
first major septal and diagonal. D1 has an instent 70% take-off stenosis.
LCx: Co-dominant system. 80% circ take-off stenosis. Scattered 30% stenosis
throughout the circ system. The L-PLA that received the SVG has a 70%
stenosis on the native vessel just at the proximal insertion of the graft.
Only a small remnant of the SVG is visible at the insertion site consistent
with occlusion.
RCA: Stent noted in proximal portion. Sub-total occlusion proximally. A
R-PDA fills faintly by L to R collaterals.
Lesion on Prox RCA: 99% stenosis.
bello ! but why not also V4R ?
ReplyDeletesaluti - Al
That would help. I was not there, so can't say why for sure. Anyway, standard 12-lead pretty much makes the diagnosis
Deletean enitre medical course in a case, thank you Dr , very usuful indeed.
ReplyDeleteThanks for the feedback!
Delete