
Written by Pendell Meyers, few edits by Smith
A woman in her 70s was woken from sleep by midsternal chest pain radiating to left arm with nausea. EMS arrived and recorded this ECG:
 |
| What do you think? |
 |
| Queen of hearts explainability image. Overall High confidence OMI. |
 |
| Improved, but still some signal of posterior OMI. Compared to prior, this suggests some improvement in TIMI flow of the culprit artery. |
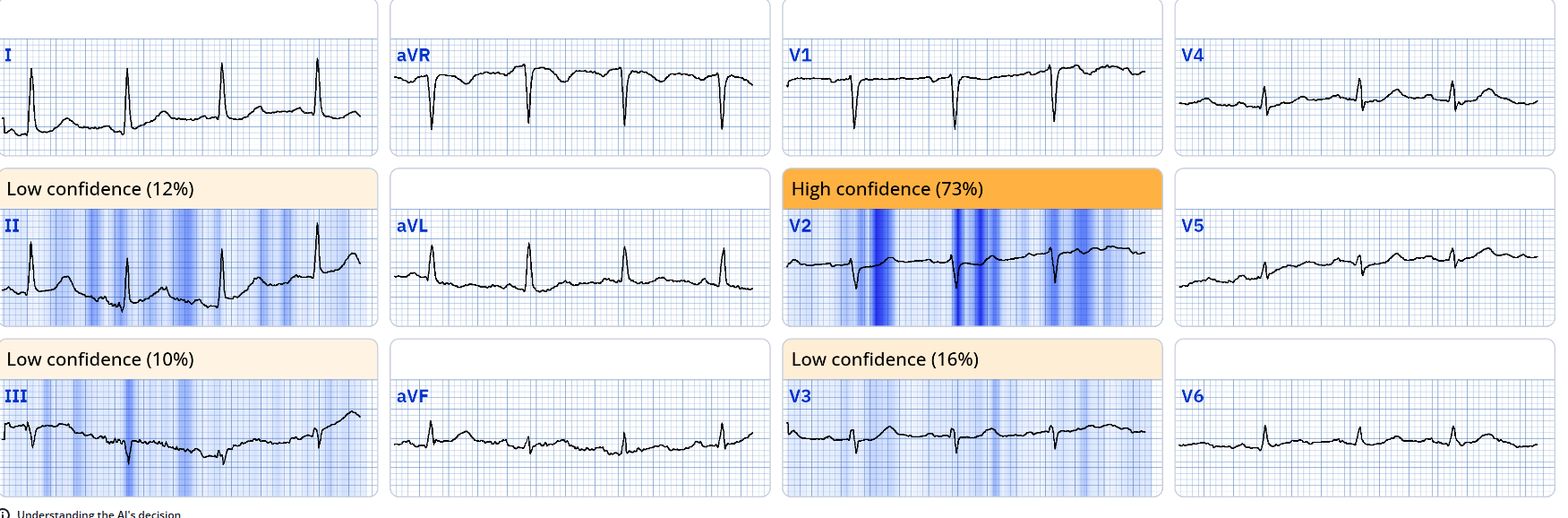 |
| Queen of Hearts explainability image showing the diagnostic findings in V2. She still gives an overall interpretation of OMI with High Confidence |
Smith: Although it is improved, it still shows OMI findings. The Queen of Hearts assesses each ECG by itself, without reference to the previous ECG. And she also does not know that the symptoms are improved. So she cannot say that there is evidence of reperfusion, whether partial or complete.
In the future, she will compare with serial ECGs and previous ECGs. Just not yet.
We can say that this is at least a partially reperfused OMI. 33% of STEMI are reperfused by the time of angiography. There are stubborn people on Twitter who think that since the artery is open at angiography, we should never have called it OMI and that the patient should not need to go for emergent angiogram. They do not understand that OMI and STEMI are the same pathophysiology, and that 1/3 of either kind will open up spontaneously.
We can't know at the time of presentation in which patients the artery will open and in which it will not; therefore, they all need cath lab activation. And they are still OMI at presentation even if the artery is open by the time of angiogram.
It is hard for me to believe how often I need to spell this out to these skeptic. Very frustrating. They hold STEMI (-) OMI to a much higher standard than they hold STEMI (+) OMI.
Angiogram was done rapidly after arrival to the ED:
Culprit mid LCX 90% TIMI 3 flow, PCI performed with resultant TIMI 3 flow.
 |
| Pre-intervention Exact TIMI-flow is uncertain. TIMI-2 vs. TIMI-3 |
{kind=link}
 |
| Post-intervention |
{kind=link}
First troponin T returned at 17 ng/mL (within normal limits using the cutoff of 20 ng/mL)

Echocardiogram:
EF 42%
Moderate hypokinesis of the mid anterolateral and apical lateral myocardium
Final diagnosis by the cardiologist was "STEMI" despite never meeting STEMI criteria.
Smith: Pendell and I have data that shows that the final diagnosis of "STEMI" vs. "NSTEMI" does not depend on presence or absence of ST Elevation, or Presence or absence of OMI.
In fact, the final diagnosis depends on whether the patient gets a short or long door to balloon time.
- Knowing that today's patient was awakened by new-onset, severe CP (Chest Pain) — Did you recognize the need to activate the cath lab as soon as you saw today's initial ECG?
- Were you at all reluctant to activate the cath lab because STEMI criteria are not satisfied on this initial EMS ECG?
- Why do you think the repeat ECG looked better than ECG #1?
- Despite improvement in both the ECG and the patient's symptoms — Did you still feel prompt cath was needed after seeing ECG #2?
-USE.png) |
| Figure-1: Comparison between the initial EMS ECG and the repeat ECG in the ED. |
- The history in today's case is classic for an acute cardiac event — as this older woman was awakened from sleep by chest pain radiating to her left arm with nausea.
- Given this history, and after recognizing that the rhythm in ECG #1 was sinus (upright P waves in lead II — with a constant and normal PR interval) — my "eye" was immediately drawn to lead III (the 1st lead within the RED rectangle in Figure-2). Given small size of the QRS complex in lead III — there is no way that the disproportionately "hypervoluminous" T wave in this lead could be normal.
- Confirmation that the T wave in lead III was indeed hyperacute — was immediately forthcoming from the finding in lead aVL of reciprocal ST-T wave depression (within the 2nd RED rectangle).
- My "eye" was next drawn to the other 2 inferior leads ( = leads II and aVF — within the 2 BLUE rectangles in Figure-2) — which, while not as flagrantly abnormal as the T wave in lead III — still show "bulkier"-than-they-should-be T waves, considering modest size of the QRS in these leads (BLUE arrows in leads II and aVF). In the context of the hyperacute T wave in lead III, in association with reciprocal ST depression in lead aVL — I interpreted the T waves in leads II and aVF as also hyperacute.
- Finally — Any doubt that could possibly have remained was immediately removed on seeing the QRST appearance of leads V2 and V3 in the chest leads (within the last 2 RED rectangles in Figure-2). These 2 chest leads show: i) Abrupt early transition to a surprisingly tall R wave already by lead V2; — and, ii) Shelf-like flat ST depression with terminal T wave positivity that clearly indicates posterior OMI (RED arrows in these leads).
- IMPRESSION of ECG #1: In this older woman who presents with severe new CP — this ECG picture is absolutely diagnostic of acute infero-postero OMI (with need for prompt cath with PCI).
- To Emphasize: There is nothing during the process of further evaluation that would have altered the decision to activate the cath lab. No matter what serial ECGs or Troponins might have shown — the need for prompt cath would have remained. So WHY wait?
- The still all-too-prevalent mindset of not performing acute cardiac catheterization unless ECG criteria for STEMI are met — needs to change. The clinical question that should be asked is not whether STEMI criteria are met — but rather whether the history and ECG suggest that an acute cardiac event is actively evolving (regardless of whether or not "enough" ST elevation is present to qualify as a stemi ).
- That the clinicians involved in today's case understood this KEY point — is evident from the fact that the cardiologist's final diagnosis was "STEMI", despite ECGs never meeting STEMI criteria.
- As per Drs. Meyers and Smith — whether the final diagnosis is "STEMI" vs "NSTEMI" primarily depends on whether the door-to-balloon time is long or short. The wisdom conveyed in this teaching message is powerful! (ie, IF the interventionist recognizes ECG findings of acute OMI before enough time has passed to allow ST elevation to develop — then successful PCI will mean that the "culprit" artery will be opened, and ST elevation will never develop).
- Waiting for ST elevation to develop when the diagnosis of acute OMI is secure — is waiting too long (as would have been the case had today's ED physician and cardiologist delayed cardiac catheterization).
- As emphasized by Dr. Smith in the November 8, 2024 post — as many as 1/3 of all acute STEMIs reperfuse spontaneously before treatment is implemented. Clinically we can usually tell when such spontaneous reperfusion occurs — because: i) The patient's CP resolves (or at least decreases); — and, ii) ST elevation resolves (or at least decreases) — and reperfusion T waves may be seen.
- In today's case — the patient felt better at the time ECG #2 was recorded. Side-by-side comparison between ECG #1 and ECG #2 in Figure-2 — clearly shows this improvement in patient symptoms corresponds to comparable improvement in the hyperacute inferior lead T waves and reciprocal changes in lead aVL.
- In the chest leads — Note that the surprisingly tall R waves in leads V2,V3 are no longer present in the repeat ECG! (PEARL: Early transition with inappropriately tall anterior R waves is a "Q wave equivalent" sign when there is posterior OMI — such that I interpreted resolution of the tall R waves in V2,V3 as further indication of posterior wall reperfusion).
- CONCLUSION: It is virtually certain that there has been some amount of spontaneous reperfusion at the time ECG #2 was recorded.
- BOTTOM Line: By history, with correlation to serial ECGs (as well as to the elevated Troponin values) — We have diagnosed an acute infero-postero OMI. So while it is good that the patient feels better following ASA and nitroglycerin — as well as good that the acute ST-T wave changes seen in ECG #1 have improved in ECG #2 — the patient remains at high-risk of spontaneous reocclusion. Prompt cath with PCI is needed to prevent this (and to optimize outcome).
-USE.png) |
| Figure-2: I've labeled the first 2 ECGs in today's case. |
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.