
Written by Pendell Meyers
Two patients with acute chest pain.
Do either, neither, or both have OMI and need reperfusion?
Patient 1:

Patient 2:

Patient 1:
A man in his 40s with minimal medical history presented with acute chest pain radiating to his R shoulder.
Triage ECG:

 |
| Slightly different, with less TWI in inferior leads this time. |
He was discharged home.
Patient 2
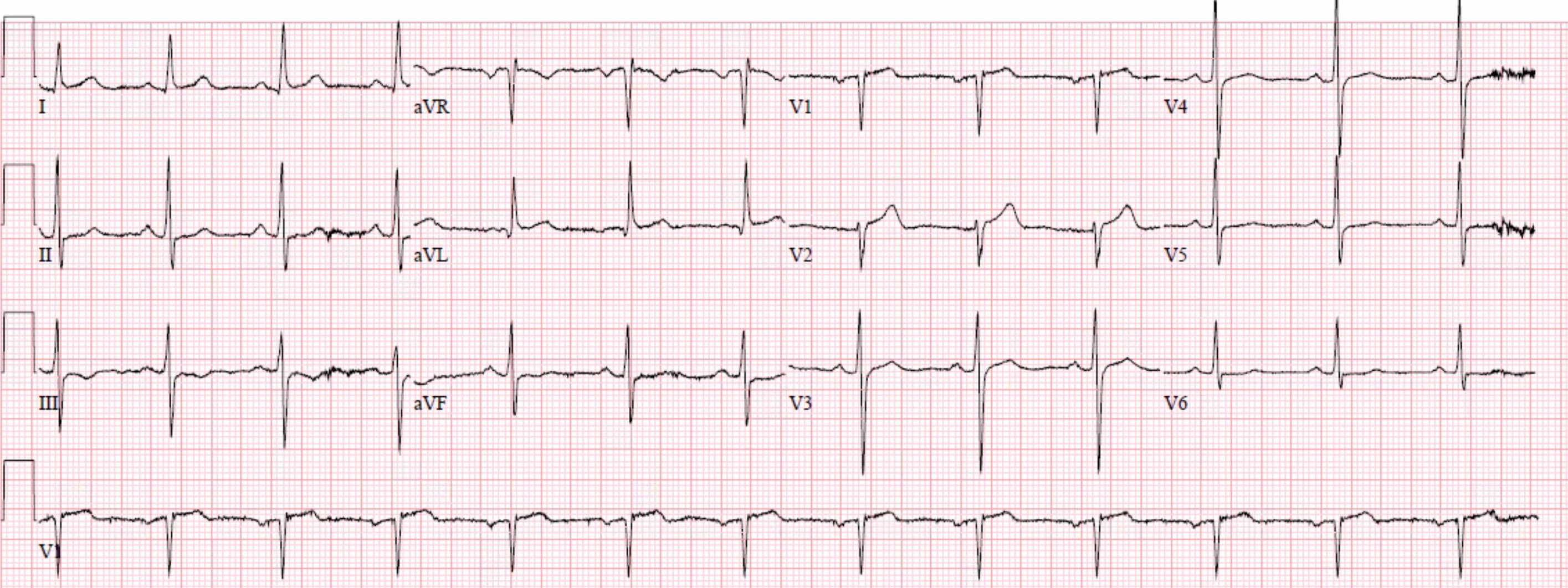
A man in his 50s with history of CAD and prior PCI, diabetes, presented with acute constant chest pain for the past few hours. Described as a dull ache, 6/10 in severity.
Triage ECG:

His disease included 70% prox LAD, 80% distal LAD, 10% in-stent stenosis in the distal LCX, 70% OM1, 70% OM2, and 60% prox RCA.
Three troponins were undetectable.
Here is another ECG later in his stay:


Compare the ECGs above with two cases of true high lateral OMIs:




How can we identify the top 2 above as false positives?
1) Use the Queen of Hearts
2) It is very difficult to explain and requires a lot of pattern recognition experience and skill. Dr. Smith identified both correctly, and so did the Queen.
3) Dr. Smith explanation: all I can say is that there is plenty of QRS voltage and that the ST segments, though elevated, have a lot of upward concavity or reciprocal downward concavity. The ST depression in V4-V6 makes this particularly difficult and hard to ascertain that it is a mimic!
4) Compare with the bottom 2 cases:
Top: small voltage QRS and straight ST segments
Bottom: ischemic appearing ST Depression in V2-V6
See these other relevant cases:
Quiz post: do either or both of these patients have high lateral OMI / South African flag sign?
True Positive ST elevation in aVL vs. False Positive ST elevation in aVL
Even when the story is obvious, with intractable pain, the STEMI paradigm can cause preventable delays
Click here to sign up for Queen of Hearts Access
- For clarity in Figure-1 — I've reproduced the initial ECGs from Patients #1 and #2 in today's case.
-USE%20copy.png) |
| Figure-1: The initial ECGs for Patients #1 and #2 in today's case. |
The above said — I’ll offer the following perspective:
- What really “counts” in a patient who presents to the ED with new CP is whether or not there is an acute, ongoing OMI for which prompt cath with reperfusion will save myocardium (and potentially save a life). This means that some of the patients who present with new CP may have underlying coronary disease from prior events (ie, the multi-vessel disease of Patient #2 in today’s case).
- While I was skeptical after seeing the ECGs in Figure-1 that the 2 patients in today’s case were having an acute OMI (for reasons similar to those highlighted by Dr. Smith above) — I fully acknowledge that I was not 100% certain there was no OMI after seeing the initial tracings. And, we want to get as close to 100% certainty as possible — so additional evaluation (ie, troponins, serial tracings, comparison with prior tracings — and at times, cardiac catheterization) — are all at times appropriate until you can be more certain.
- Although not perfect — the QOH application can be reassuring. Together with the illustration of numerous cases on Dr. Smith’s ECG Blog — our hope is to facilitate rapid identification when acute OMI can be immediately diagnosed by history and the initial ECG. And, although prudence is advised until one attains that greater certainty that an acute event is not ongoing — our hope is that some diagnostic cardiac catheterizations that are not needed can be avoided by the tips and insights provided on this ECG Blog
- That said, today’s cases are tough — because both initial ECGs manifest ST elevation with ST depression in oppositely-directed leads — and both manifest taller-than-expected T waves in lead V2 — as well as some unexpected ST depression.
- LVH may further complicate assessment for OMI. As per Dr. Smith — criteria for LVH are satisfied in Patient #2 (ie, R > 20 mm in lead II). Although voltage criteria may fall a bit short for LVH in Patient #1 — the ST-T wave in lead V6 looks typical for LV “strain”. (For more on LVH — See My Comment in the June 20, 2020 post in Dr. Smith’s ECG Blog).
- Bottom Line for Me: Were I in the ED — I would not have been certain from just the initial ECG that there was no OMI, until I obtained more information. I learn from knowing Drs. Smith, Meyers & QOH were certain sooner than I was.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.