
Written by Pendell Meyers
A woman in her 70s had acute chest pain and called EMS.
On arrival, EMS recorded relatively normal vital signs and this EMS ECG:
 |
| What do you think? |
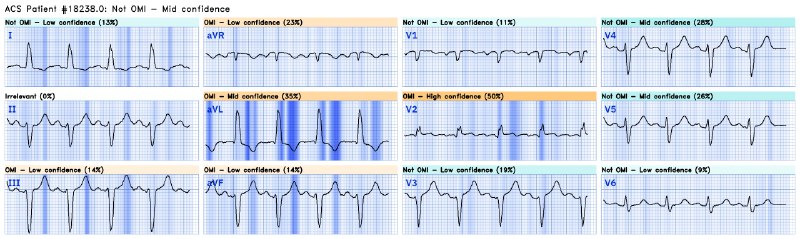
Interpretation: diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Because the reciprocal area from V2-V4 is the posterior wall, many anterior OMIs do not have clear reciprocal findings on the standard 12 leads.
Here is the Queen of Hearts interpretation:

This ECG was transmitted to the nearest PCI center, where it was simply called "Not STEMI, just follow your protocol." So the cath lab was not activated.
The EMS crew recorded another ECG about 10 minutes later (unknown if pain changed):
 |
| New LAFB. Now it even meets STEMI criteria, and HATWs continue to inflate. Ongoing OMI. |


Again, it was sent to the PCI center where they said "No STEMI, just transport."
Approximately 20 minutes later, EMS recorded another ECG (no info available about presence/absence of pain unfortunately):
 |
| Interval improvement / reperfusion. The T waves have deflated significantly to the point that they could be within normal limits. V2 still has a touch of STE and terminal T wave inversion, which is of course indicative of reperfusion. LAFB remains. |

 |
| Notice that she overall thinks that the ECG is not diagnostic of OMI (as it is close to normal, between occlusion and reperfusion sequences, as she has no ability to judge serial ECGs together yet), but she is still very concerned about lead V2 individually. |
The patient arrived to the ED and had troponins drawn which eventually resulted elevated (values not available).
The time from arrival to cath is not clear, but at least several hours delay. At delayed cath she was found to have a culprit mid LAD lesion 95% at time of cath (no TIMI flow available), for which PCI was performed.
No further ECGs were recorded.
The patient survived with unknown long term outcome.
She was very lucky to have spontaneous reperfusion.
Get access to Queen of Hearts here:
https://share-eu1.hsforms.com/18cAH0ZK0RoiVG3RjC5dYdwfyfsg
MY Comment, by KEN GRAUER, MD (1/3/2024):
- For clarity, and to facilitate comparison of these serial ECG changes — I've put the 3 tracings in today's case together in Figure-1.
- Unfortunately — much data from this case is unavailable. What we do know — is that despite prompt EMS transfer to the nearest PCI facility — the series of ECGs recorded by the EMS team was interpreted as "Not a STEMI — No need for cath lab activation."
-USE.png) |
| Figure-1: Comparison between the 3 ECGs in today's case. |
- As per Dr. Meyers, given the history of new CP — ECG #1 is diagnostic of acute anterior OMI from LAD occlusion until proven otherwise. The rSr' complexes in leads V1 and V2 are unusual in lacking terminal S waves in lateral leads I and V6 that are required for incomplete RBBB. While the R' positivity in lead V2 (in the absence of any similar-looking deflection in either V1 or V3) might reflect a component of electrode lead misplacement — even if present, this would not negate the ST elevation that we see in lead V2, as well as in lead V1.
- As per Dr. Meyers — hyperacute T waves are clearly seen in leads V2,V3,V4 (within the BLUE rectangles) — in the form of disproportionately increased T wave amplitude — with each of these T waves being "fatter"-at-their-peak and wider-at-their-base than expected given QRS dimensions in these leads.
- In the context of hyperacute T waves in leads V2,V3,V4 — neighboring leads V1 and V5 are also abnormal (lead V1 with an abnormal amount of ST elevation for this initial chest lead — and lead V5 with a T wave smaller than the T wave in lead V4, but still "fatter"-than-expected at its T wave peak).
- As per Dr. Meyers — ST segment straightening in each of the inferior leads qualifies as supportive reciprocal change.
- BOTTOM Line: In this patient with new CP, the above described abnormal findings in ECG #1 — clearly qualify as indication for prompt cath lab activation. Proof of this justification was eventually forthcoming when cardiac cath was finally performed — confirming total mid-LAD occlusion.
- The QRS complex has clearly widened in ECG #2 — now measuring between 0.11-0.12 second. That said — it is difficult to classify the type of conduction defect that has developed. The QRS is not quite wide enough for LBBB — and the all upright QRS in lead V6 that is expected with LBBB is lacking. The markedly leftward frontal plane axis most closely resembles LAHB (Left Anterior HemiBlock) — though when isolated, LAHB does not usually widen the QRS by as much as we see the QRS widened in Figure-1.
- Given the significant QRS widening in ECG #2 — I was not sure how to assess limb lead ST-T wave appearance in comparison to ST-T wave appearance that we see when the QRS is narrow in ECG #1.
- That said — lead-by-lead comparison between ECG #1 and ECG #2 with regard to chest lead ST-T wave appearance clearly confirms ongoing acute LAD occlusion because: i) Lead V1 now shows ST coving and more ST elevation in ECG #2, than was present in ECG #1; — and, ii) Even accounting for the QRS widening — T waves in leads V2-thru-V6 all look more hyperacute (taller and "bulkier" than they were in ECG #1).
- BOTTOM Line: We see a new infarction-related conduction defect in ECG #2 — in association with increasingly hyperacute T waves in all chest leads. In this older woman with new chest pain — I find it difficult to justify not activating the cath lab.
- NOTE: Heart rate of the sinus rhythm in ECG #1 and ECG #2 is virtually the same (about 100/minute). This is relevant, because the conduction defect is therefore not rate-related. Instead — QRS widening is almost certainly related to acute ischemia from extensive infarction, thereby suggesting another adverse prognostic factor.
- Of note — the conduction defect persists in ECG #3.
- Isn't it EASIER to compare serial tracings when you put tracings side-by-side (as is done in Figure-1) — and then compare tracings by looking lead-by-lead?
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.