
Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. This episode of chest pain began 3 hours ago and was persistent even at rest.
Triage ECG at Time = 0:

Smith: I am suspicious for posterior OMI due to ST depression in V2 and V3
Baseline EKG (several months prior):

Smith: Now I am even more suspicious of posterior OMI, as the baseline ECG has normal ST elevation in V2 and V3
ECG Interpretation:
The triage ECG shows sinus rhythm with subendocardial ischemia pattern as seen by STD in V3-V6, II, III, and aVF, with small reciprocal STE in aVR.
The baseline ECG is basically normal with no ischemia.
Here is what the Queen of Hearts says about the Baseline ECG:
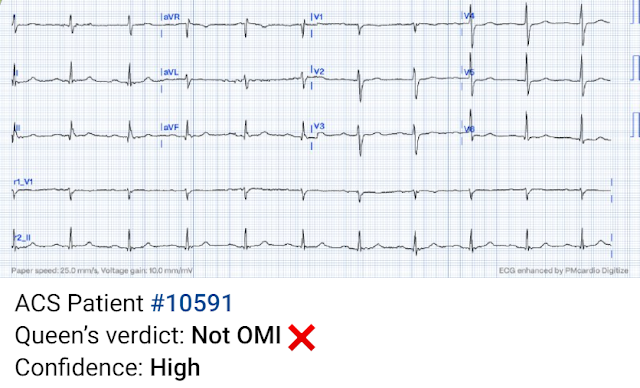

Active chest pain triage ECG also read as not OMI:

She says "not OMI", but she does not have access to the baseline ECG. In the future, we will be able to have her compare with previous and serial ECGs.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). Troponin was ordered.
Time = 45 minutes: hs Troponin I returns at 15 ng/L (within normal upper reference range of 20)
Time = 1.5 hours: Second troponin increased to 26 ng/L.
Because the troponin rose (not due to pain resolution), the ECG was repeated:
 |
| More severe subendocardial ischemia vs. posterior OMI. In my opinion, I think it looks more like subendocardial ischemia. |
Smith: I think it looks more like posterior OMI. When Pendell and I are coding ECGs for the Queen's training, this is one category: "Definite ischemia, difficult to differentiate between posterior OMI and subendocardial ischemia."
Queen of Hearts now thinks that this one looks like posterior OMI, since the STD does appear worst in V3-4:

None of this seems to have been understood by the EM doctor or the cardiologist who was consulted. He was diagnosed as NSTEMI. He had already been given aspirin and heparin. For the ongoing pain and rising troponin, instead of taking the patient to the cath lab as all NSTEMI guidelines in the world recommend, the patient was given morphine and nitroglycerine drip and admitted.
Smith: Read more about the danger of morphine. In our opinion it should not be given in ACS unless you are committed to the cath lab. We have shown that it is highly associated with delays to cath lab in patients who need the cath lab emergently.
Time = 3 hours: the next troponin returns at 60 ng/L. The notes now refer to the patient being in cardiogenic shock, on pressors. Repeat ECG:

Meyers: This is the first time I have ever seen this combination! LBBB with de Winter hyperacute T waves in leads V2-V5. It can also be describe as LBBB with precordial swirl pattern, with likely excessive STE / HATW in V1/2 with reciprocal excessive STD in V5/6. II, III, and aVF have inappropriate STD which is likely reciprocal STD.
If you are not certain what "Swirl" is, see here:
The Queen, who has trained on some LBBB OMI and some non-LBBB de Winter ECGs, for the first time ever seeing them in combination, instantly diagnoses OMI with high confidence and highlights the de Winter pattern in the LBBB:


Finally the patient was taken to the cath lab at around 4.5 hours from presentation, where he was found to have an acute thrombotic LAD occlusion which was stented with resulting TIMI 3 flow, but still the patient was in severe cardiogenic shock. An Impella was placed for cardiac output augmentation. Left ventriculogram revealed severe apical and anterior dyskinesis with moderate generalized hypokinesis. LV ejection fraction was noted to be roughly 20%.
Over the course of the next 24 hrs he developed worsening refractory cardiogenic shock and expired.
Learning Point:
Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. Yet this is rarely followed, and patient outcomes like this are the result once in a while.
This patient had persistently ischemic ECGs with subendocardial ischemia pattern and active ACS symptoms. While subendocardial ischemia pattern can be due to any possible reason for supply/demand mistmatch in infinite clinical scenarios, this patient's scenario was acute chest pain consistent with ACS. Therefore it means acute type 1 ACS plaque rupture with impeded flow and impending full occlusion until proven otherwise.
Then, the patients third ECG showed a very rare combination of de Winter T waves happening during LBBB. I have not yet seen any case report of this combination.
The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. It is already approved in Europe.
YOU HAVE THE OPPORTUNITY TO GET EARLY ACCESS TO THE PM Cardio AI BOT!! (THE PM CARDIO OMI AI APP)
If you want this bot to help you make the early diagnosis of OMI and save your patient and his/her myocardium, you can sign up to get an early beta version of the bot here. It is not yet available, but this is your way to get on the list.
Some references on de Winter morphology:
1. de Winter RJ, Verouden NJ, Wellens HJJ, Wilde AA. A new ECG sign of proximal LAD occlusion. N Engl J Med. 2008;359:2071–2073.
2. Verouden NJ, Koch KT, Peters RJ, Henriques JP, Baan J, van der Schaaf RJ, Vis MM, Tijssen JG, Piek JJ, Wellens HJ, Wilde AA, de Winter RJ. Persistent precordial “hyperacutic” T-waves signify proximal left anterior descending artery occlusion. Heart. 2009;95:1701–1706.
3. Morris N, Body R. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. Eur J Emerg Med. 2017;24:236–242.
4. Goebel M, Bledsoe J, Oxford JL, Mattu A, Brady WJ. A New ST-segment elevation myocardial infarction equivalent pattern? Prominent T wave and J-point depression in the precordial leads associated with ST-segment elevation in lead aVR. Am J Emerg Med. 2014;32:e5–e8.
5. Hayakawa A, Tsukahara K, Miyagawa S, et al. The reappearance of de Winter's pattern caused by acute stent thrombosis: A case report. J Cardiol Cases. 2022;25(6):404-407. Published 2022 Feb 20. doi:10.1016/j.jccase.2022.01.006
2. Verouden NJ, Koch KT, Peters RJ, Henriques JP, Baan J, van der Schaaf RJ, Vis MM, Tijssen JG, Piek JJ, Wellens HJ, Wilde AA, de Winter RJ. Persistent precordial “hyperacutic” T-waves signify proximal left anterior descending artery occlusion. Heart. 2009;95:1701–1706.
3. Morris N, Body R. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. Eur J Emerg Med. 2017;24:236–242.
4. Goebel M, Bledsoe J, Oxford JL, Mattu A, Brady WJ. A New ST-segment elevation myocardial infarction equivalent pattern? Prominent T wave and J-point depression in the precordial leads associated with ST-segment elevation in lead aVR. Am J Emerg Med. 2014;32:e5–e8.
5. Hayakawa A, Tsukahara K, Miyagawa S, et al. The reappearance of de Winter's pattern caused by acute stent thrombosis: A case report. J Cardiol Cases. 2022;25(6):404-407. Published 2022 Feb 20. doi:10.1016/j.jccase.2022.01.006
6. Guidelines are rarely followed: Lupu L, Taha L, Banai A, Shmueli H, Borohovitz A, Matetzky S, Gabarin M, Shuvy M, Beigel R, Orvin K, Minha S ’ar, Shacham Y, Banai S, Glikson M, Asher E. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardial infarction patients. Clin Cardiol [Internet]. 2022;Available from: https://onlinelibrary.wiley.com/doi/10.1002/clc.23781
7. Morphine is dangerous: Bracey, A. Meyers HP. Smith SW. Wei L. Singer DD. Singer A. Association between opioid analgesia and delays to cardiac catheterization of patients with occlusion Myocardial Infarctions. Academic Emergency Medicine 27(S1): S220; May 2020. Abstract 556.

"MY Take" — on deWinter T Waves:
===================================
MY Comment, by KEN GRAUER, MD (11/3/2023):
===================================
Distinction between posterior OMI vs deWinter T waves — is sometimes easy, but sometimes surprisingly difficult. And so I found today’s case especially interesting and insightful regarding the differentiation between these 2 entities.
- In the interest of highlighting some additional Learning Points — I’ve made 2 figures that compare today’s tracings — beginning with Figure-1.
QUESTION:
- At what point in today’s case is the need for prompt cath confirmed?
- — HINT: Consider the 2 tracings shown in Figure-1.
-USE.png) |
| Figure-1: Comparison of today's initial ECG — with a baseline ECG done several months earlier. |
The Point that Confirms the Need for Prompt Cath:
The history in today's case is that of a man in his 70s with known coronary disease (s/p LCx stenting ~2 years earlier). He presented with recent angina that evolved into a 3-hour episode of persistent CP unrelieved by rest.
- As per Drs. Franks, Meyers & Smith — the initial ECG is clearly abnormal, with multiple leads showing ST segment straightening, slight ST depression and terminal T wave positivity.
- Regardless of whether ECG #1 reflects DSI (Diffuse Subendocardial Ischemia) or posterior OMI — this patient is clearly at great risk with need for rapid decision-making to determine IF he is actively evolving an acute event (ie, Quick search for a prior tracing — and — Repeating the initial ECG within no more than 15-20 minutes!).
Unfortunately — 1.5 hours passed until the ECG was finally repeated ...
- But a baseline ECG from several months earlier was found ( = ECG #2 — shown in Figure-1). As per Drs. Franks, Meyers & Smith — Comparison of the 2 tracings shown in Figure-1 clearly reveals marked changes in multiple leads.
- BOTTOM Line: Given the history of a man in his 70s with known coronary disease + new persistent CP + an initial ECG strongly suggestive of DSI (if not acute posterior OMI) with ST-T wave changes that are indisputably new from a previous tracing done a few months earlier — the need for prompt cath is clearly confirmed the moment this patient's baseline ECG is found! Neither troponin values nor additional ECGs are needed for making the decision to immediately activate the cath lab.
=================================
We've previously published many cases illustrating deWinter T waves (Please see My Comment at the bottom of the page in the April 17, 2023 post of Dr. Smith's ECG Blog — in which I review ECG findings from the original 2008 manuscript by deWinter et al). I repeat below some of my observations from that post regarding deWinter T waves:
- Many of the cases I've seen do not fit strict definition of “deWinter T waves” (as described by deWinter et al) — in that fewer than all 6 chest leads may be involved — J-point ST depression is often minimal (if present at all) in many of the chest leads — and, the number of leads that manifest giant T waves is limited.
- ECG changes in many of the cases I've seen are not “static” until reperfusion (as had been initially reported in 2008 by deWinter et al.).
- I believe there is a spectrum of ECG findings, that in the setting of new-onset cardiac symptoms is predictive of acute LAD occlusion as the cause. I suspect that to a large extent — what is seen on ECG depends greatly on when during the process the ECG is obtained.
What Today's Case Adds to Our Understanding:
As I noted at the beginning of My Comment — it is sometimes easy to distinguish between posterior OMI vs deWinter T waves. But sometimes (such as in today's case!) — it may be surprisingly difficult at an early point in the process!- The spectrum of ECG findings potentially associated with deWinter T waves not only depends on when during the process the ECG is obtained — but it also depends on what the baseline ECG looks like!
I fully acknowledge that I did not predict that ECG #1 was the initial tracing in what was to evolve into a definite deWinter T wave pattern predictive his LAD OMI. In retrospect — there were clues:
- PEARL #1: As you take another LOOK at the 2 tracings in Figure-1 — Note that compared to the prior tracing that showed diffuse ST-T wave flattening — ECG #1 shows emerging T wave peaking in all 6 chest leads (extending out to leads V5 and V6!). Although posterior OMI is often characterized by terminal T wave positivity — this usually does not extend out to lead V6.
- Although typical deWinter T waves show a rapidly upsloping of the ascending T wave limb — Seeing how flat all chest lead ST segments were in the baseline ECG should have clued me into not expecting rapidly upsloping T wave ascent early in the process.
- PEARL #2: The fact that there is no sign of acute inferior OMI in ECG #1 — is a feature against there being posterior OMI. To Emphasize: The lack of ECG findings suggestive of inferior OMI does not rule out the possibility of posterior OMI (ie, There can be isolated posterior OMI — as may occur with Obtuse Marginal OMI) — but it is clearly more common to see ECG findings suggestive of both inferior and posterior involvement, than of isolated posterior OMI.
I thought it interesting to follow the evolution over ECG #3 (done 1.5 hours after ECG #1) — and then ECG #4 (done 3 hours after ECG #1) — which I trace out in Figure-2 that puts all 3 of the ECGs done on the day this patient presented together.
- I fully acknowledge that on seeing ECG #3 — I became more "convinced" the patient was evolving acute posterior OMI — because of what I interpreted as maximal ST-T wave depression in leads V3 and V4.
- PEARL #3: I missed the clue in ECG #3 — that as the amount of chest lead J-point ST depression was becoming greater — that the slope of the ascending T wave was clearly getting steeper (compared to ECG #1) — at the same time the pearked terminal T wave positivity was increasing (compared to ECG #1) in all 6 chest leads.
- PEARL #4: Looking just at the ST-T waves in ECG #4 — Isn't the evolution of ST-T wave changes over the course of the 3 tracings in Figure-2 now perfectly characteristic of deWinter T waves? (ie, marked J-point ST depression in leads V3-thru-V6 — with steep upsloping ascending T waves that culminate in disproportionately tall, peaked T waves across the chest leads).
- PEARL #5: As per Dr. Meyers — Today's case adds a deWinter T wave variant that I had not previously seen = LBBB with deWinter T waves. In my "series of 1" — today's patient expired, suggesting a grave prognosis for this combination.
Closing NOTE: As interesting as I find it to go back and trace the subtle clues suggesting the LAD rather than the LCx as the "culprit" artery in today's case — Regardless of what the culprit artery turned out to be in today's case — prompt cath should have been done as soon as the baseline tracing was found.
-USE.png) |
| Figure-2: Comparison of the 3 ECGs done during this patient's admission. |
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.