
Imagine you just started your ED shift. It's a busy Friday afternoon. Triage is backed up, and 10 minutes into your shift one of the ED nurses brings your several ECGs that has not been overread by a physician.
All of the patients presented with chest pain, and they are all in triage.
Which, if any, of these patients has OMI, with myocardium at risk and need for emergent PCI?
ECG#1

ECG#2

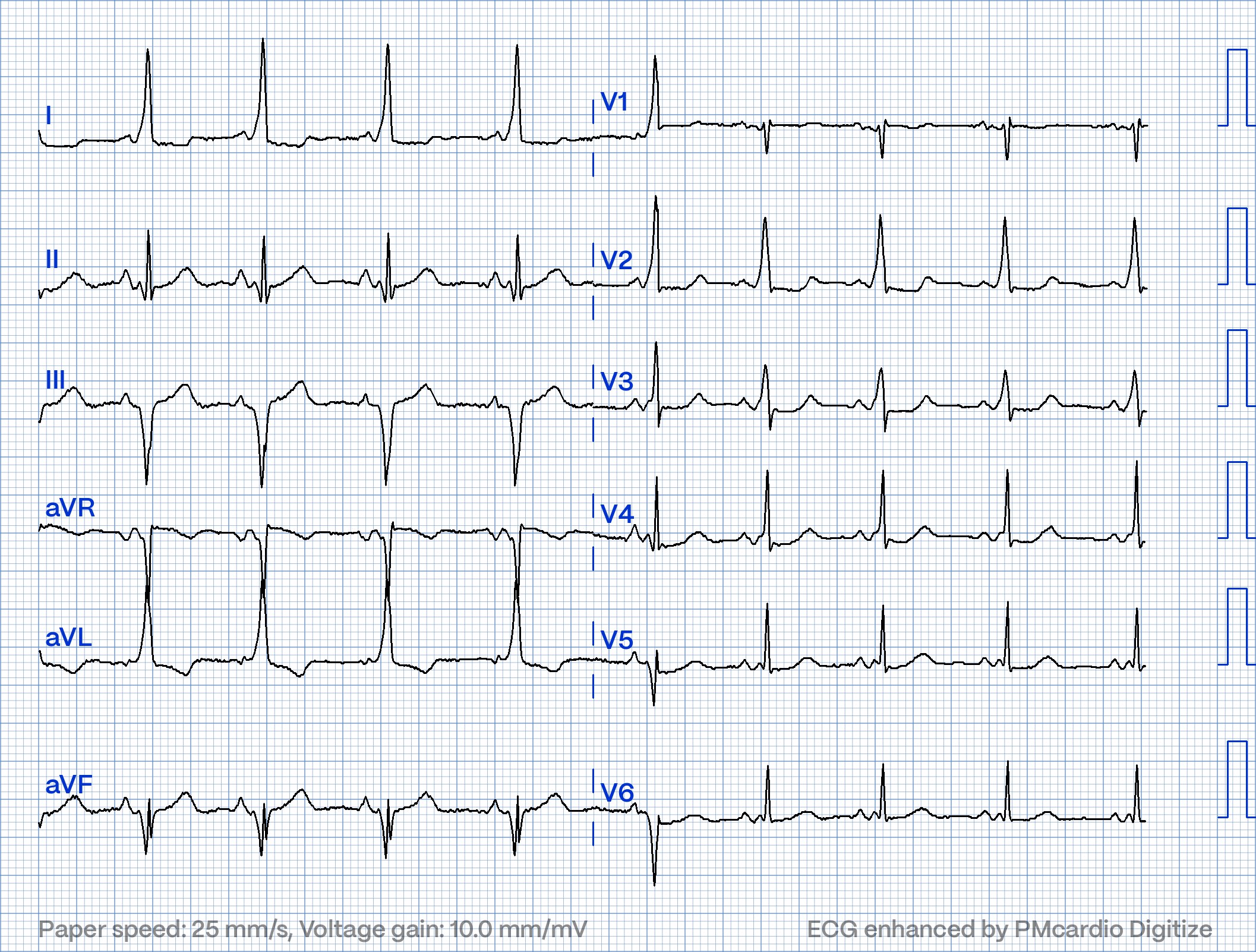
ECG#3

ECG#4

ECG#5
See outcomes of all 5 below, with the Queen of Hearts AI Bot interpretation.
YOU TOO CAN HAVE THE PM Cardio AI BOT!! (THE PM CARDIO OMI AI APP)
If you want this bot to help you make the early diagnosis of OMI and save your patient and his/her myocardium, you can sign up to get an early beta version of the bot here. It is not yet available, but this is your way to get on the list.
ECG #1: There is sinus rhythm, narrow QRS complexes. There is however definite pathologic ST-T changes with hyperacute T waves in leads II, III and aVF with ST-segment straightening and increased area under the T-waves. There is inappropriate ST-depression in lead V2. There is some down sloping ST-segment and T wave inversion in lead aVL. The findings are diagnostic of inferior and posterior wall OMI. The patient was referred immediately for cath which revealed RCA occlusion that was stented.
How did the Queen of Heart AI model perform? True Positive

ECG#2: Also sinus rhythm. There is impressive ST-elevation widespread in many leads with no real reciprocal change. There is ST depression in V1. Remember, in diffuse subendocardial ischemia with widespread ST-depression there may be ST-E in leads aVR and V1. Here the case is the opposite(!) The STE vector produces ST depression in leads aVR and V1, and thus this ST depression must be viewed as mirroring/reflecting (reciprocal to) the widespread nonischemic STE. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. There are also J-waves. The ECG just doesn't look ischemic.
Using the Smith 4 variable LAD occlusion formula gives a value of 17,7. This is in line with likely ST elevation of non-ischemic origin. (RR 1100ms. QT 400ms. QTc 381ms. QRS V2 26mm. STE @60 ms after J point V3 4mm. R wave V4 9mm)
CT of the coronary arteries showed no lesions. Calcium score 0. Troponin I rose to >48.000ng/L. MR showed findings consistent with extensive myopericarditis.
How did the Queen of Heart AI model perform? False positive.

ECG#3 Again an ECG with sinus rhythm, narrow QRS complexes and ST-T changes. There again are well formed R-waves. There is ST elevation lead V2-V6 with T wave inversion. ST-elevation with T wave inversion obviously could be ischemic in nature. (E.g. reperfused/subacute OMI) However, there are very prominent J waves. The initial description of a prominent J wave was made by Osborn in 1938 in a hypothermic patient. Prominent J waves of this morphology thus are called Osborn waves. Severe hypothermia not uncommonly has accompanying T waves inversions. Another frequent feature of hypothermia is atrial fibrillation (not seen in this case) Core temperature of this patient was 29,5 Celsius. Troponins were negative in serial blood tests.
Smith comment: This ECG is also consistent with Benign T-wave Inversion. See these multiple cases.
Magnus response: VERY interesting you say that, I sadly do not have follow up ECG or patient ID on this case, so now I cannot check the repeat ECG. I do remember checking the ECG the following day and it was quite similar, but not this much pronounced findings. At that time I didn't think much about it. Maybe the main cause of the ECG-findings here then is benign T inversion and not hypothermia. Also maybe hypothermia will unmask or even accentuate BTWI findings?
How did the Queen of Heart AI model perform? False positive

ECG#4 This ECG was recorded in a patient post ROSC. There is SR. There are very pathologic ST-segment throughout the precordium with STE that could be reminiscent of brugada like morphology in the early precordial leads. (V1-V3) The QRS may appear very wide, but it is not. It is slightly more than 0,12s (three small boxes). There is ST Elevation in lead I and aVL. The axis is to the right and QRS complexes in lead I and aVL are predominantly negative suggesting LPFB. This patient at cath had a large CX occlusion with a massive troponin release. Troponin T >42.000ng/L. The patient died of cardiogenic shock within 24 hours despite mechanical circulatory support. Below the J-point is marked out showing the ST pathologic deviations.

Smith: This bizarre ECG looks like a post cardiac arrest ECG with probable acidosis or hyperkalemia in addition to OMI. What was the pH and K?
Magnus response: Upon admission to PCI center, the pH on blood gas was 6,84. Potassium 4,6. A repeat ECG at admission showed more typical OMI findings with less bizarre waveform, thus ECG #4 then likely represents acute OMI + severe metabolic derangement.
How did the Queen of Heart AI model perform? True positive

ECG#5 There is, like in ECG#1 ST-T wave changes in the inferior leads and ST depression in lead V2-V3 with tall precordial R wave by lead V2. Why is this not OMI like the first case? These ST-T changes are all secondary to abnormal depolarization. The ECG does not show any signs of ischemia. All ST-T changes are secondary to ventricular preexcitation. This is pseudo-infarct pattern from WPW.
How did the Queen of Heart AI model perform? True Negative

So, based on the above interpretations patients with ECG #1 and #4 should be considered for the cath lab.
As you can see ECG #2 and #3 were false positives for the QoH. These ECGs are difficult. It is noteworthy that ECG #2 shows a lot of ST elevation and that the AI model still does not say high confidence. The other false positive was interpreted as OMI with low confidence. With more training the AI algorithm will get even better and ECG #3 will likely be identified as not OMI. The goal in clinical practice must NOT be to never have a false positive cath lab activation, if that's your goal you will also have a lot of false negatives which is exactly what we seek to avoid.
![]()
===================================
MY Comment, by KEN GRAUER, MD (10/8/2023):
===================================
I love this case by Dr. Nossen — because of its thought-provoking concept of, "What to do with no time to lose — and multiple patients who are presenting with new chest pain?"
- In the interest of stimulating active interchange — I'll propose changing the question asked from, "Which 2 patients need to go emergently to the cath lab?" — to — "Which patient needs immediate cath? — and which other patient(s) need to be seen as soon as possible to figure out what is going on?
==============================
MY Thoughts:
The patient with ECG #1 needs immediate cath.
The patient with ECG #2 — needs to be seen as soon as this is possible.
I found ECG #3 interesting — in that I would not have guessed that this patient with new CP was hypothermic from looking at this tracing.
- I completely agree with Dr. Nossen that in this patient with new CP and sinus tachycardia with LAHB — that the T waves in each of the inferior leads are hyperacute (ie, clearly disproportionately "bulky" given size of the QRS in these leads).
- In this context — lead V2 findings of a Q wave and ST segment straightening with depression and terminal T wave positivity are diagnostic of acute infero-postero OMI — which as per Dr. Nossen was confirmed on cath.
- I would find it hard not to expedite formulating a working diagnosis by "laying my eyes on this patient" — given the complaint of "new CP" — and this ECG showing marked ST elevation (more than 5 mm in V5,V6 — and more than 2-3 mm in multiple other leads) in association with these giant positive T waves.
- I completely agree with Dr. Nossen that — this is not the ECG of acute OMI. Instead — it is perfectly consistent with acute myopericarditis given: i) Diffuse ST elevation without reciprocal ST depression; ii) ST-T wave appearance in lead II that is much more similar to ST-T appearance in lead I rather than lead III (the opposite tends to be seen with acute MI); iii) The q waves present are tiny (normal "septal" q waves in leads V5,V6); and, iv) The amount of J-point ST elevation and excessive T wave size are features that suggest myocarditis in addition to simple acute pericarditis.
- Bottom Line: Tests other than cardiac cath may be all that are needed to establish the diagnosis — but, I'd want to see a patient with this ECG as soon as would be possible.
- Prominent J waves are only present in 2 leads (leads V2,V3) — albeit much smaller J waves are seen in leads aVL and V4.
- Hypothermia is often associated with ST elevation in multiple leads — but generally not with the shape of ST elevation ending in terminal T wave inversion that we see in leads V2,V3. Seeing "rounding" of the ST segment in multiple other leads, albeit with much less ST segment deviation (ie, in leads I,II; V4,5,6) — to me was much more suggestive of a benign repolarization variant.
- The above said — this patient was markedly hypothermic ( = 29.5C°) — so the only way to verify which ECG findings were the result of a repolarization variant vs hypothermia vs a combination of both — would be to review follow-up tracings after core temperature normalized. Unfortunately — follow-up tracings are not accessible from this case.
- Bottom Line: While any patient who presents to the ED with "new CP" and an ECG showing some ST elevation and T wave inversion needs to be seen sooner-rather-than-later — I would not rush to the patient's bedside on the basis of this ECG.
I thought ECG #4 — to be a bit bizarre. I would not have sent this patient emergently to the cath lab solely on the basis of this tracing. Instead — I thought this to be a patient needing immediate attention to first figure out what is going on.
- Although there clearly is marked ST elevation in multiple leads — the QRS is widened, with slow initial activation and a morphology not typical of known conduction defects (ie, Bizarre, rounded initial deflection in V1 not typical of RBBB — minimal r wave, with slowed S wave downslope in lead I not typical of LPHB — all-too-similar-looking RS complexes in V2-thru-V6, with unusually widened initial R wave in V2).
- The rhythm is uncertain (ie, We only see 4 beats — because the same 4 beats are repeated in limb and chest leads — but in lead II there appears to be sinus bradycardia and arrhythmia plus a P wave with a PR interval too short to conduct preceding beat #1 — therefore need for a longer period of monitoring).
- Bottom Line: While fully aware that the marked ST elevation in multiple leads might indicate extensive acute and ongoing infarction — I thought the overall ECG picture was more suggestive of some toxicity and/or metabolic disturbance in need of more assessment before ordering cardiac cath. Although details from this case are not optimally available — it appears that this patient was markedly acidotic — which could be consistent with the unusual features of this ECG.
As per Dr. Nossen — ECG #5 shows sinus rhythm with WPW. I would not send this patient for immediately cath. That said, this patient did present to the ED with "new CP" — and ...
- We do not have a baseline ECG. So while true that the overwhelming majority of WPW cases I have encountered manifest "abnormal" ST-T wave changes that are due to the WPW and not the result of acute infarction — on occasion, abnormal ST-T waves in a patient with WPW may be abnormal because of acute infarction (See Dr. Smith's example in the March 1, 2012 post — of a patient with WPW and new MI that resulted in superimposed acute ST-T wave changes on top of baseline WPW findings).
- In ECG #5 — Isn't there excessive ST segment straightening with slight ST depression in leads V2-thru-V5? While possible that this ST-T wave chest lead appearance is entirely due to WPW — I'm more used to seeing some downsloping ST angulation in WPW tracings in which the QRS is predominantly positive in chest leads.
- Bottom Line: I definitely would not activate the cath lab on the basis of this tracing showing WPW. But this patient did present to the ED with "new CP" — and I thought the anterior chest lead ST segment flattening with depression a bit atypical for simple WPW. It would tremendously help to find a baseline tracing — together with a set of negative troponins to ensure that there has been no acute event.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.