
Submitted by Dr. Dennis Cho (@DennisCho), written by Jesse McLaren
A 70-year-old with no cardiac history presented with 2 hours of chest pain radiating to the neck, associated with shortness of breath. What do you think?

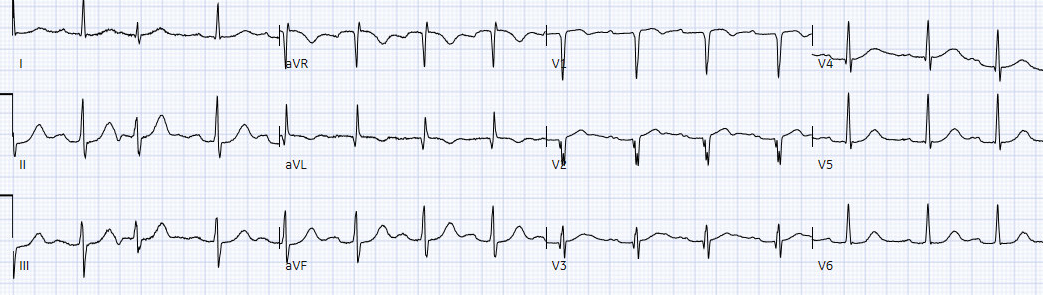
There’s normal sinus rhythm, first-degree AV block, normal axis and voltages. R wave progression is abnormal: there are Q waves in aVL/V2-3 and loss of R wave in V2. This is accompanied by minimal ST elevation in aVL/V1-V2 and more pronounced inferior reciprocal ST depression, and minimal ST depression V5-6. This is diagnostic of OMI, either proximal LAD or first diagonal.
Q wave, old infarct?
Below is the old ECG, showing that all these changes are new – including the Q waves.

While the final interpretation on the new EGC is “anteroseptal infarct, old”, the patient had developed acute Q waves after only 2 hours of ischemic symptoms. Acute Q waves are a marker of severe ischemia and a predictor for delayed reperfusion.
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. As he documented, “This patient is experiencing chest pain consistent with an acute coronary syndrome. I am concerned about these ECG findings as they may represent a subtle occlusion.” So he asked for a stat cardiology consult to consider cath lab activation.
OMI or STEMI?
Cardiology repeated the ECG, still STEMI(-)OMI but with loss of R wave in V3:
The first troponin returned at only 100 ng/L (normal <26 in males and <16 in females) – confirming that the Q waves was acute, not subacute or old. Bedside echo showed anterior regional wall motion abnormality, corresponding to ECG changes. As cardiology documented, “possible STEMI. Given ECG changes, echocardiographic findings, and typical history, code STEMI called.”
Cath lab was activated and found a 100% proximal LAD occlusion, with peak troponin I of 130,000 ng/L and EF 40% - which improved to 55% on discharge. Discharge ECG showed reperfusion T wave inversion with further loss of R wave in V3:

Discharge diagnosis was “STEMI” despite no ECG ever meeting STEMI criteria.
Paradigm shift
As Smith/Meyers wrote, while there needs to be a paradigm shift from STEMI to OMI, there are concrete steps that we can immediately take: “What should we do in the meantime while we are still stuck in the STEMI paradigm in daily practice?
First, start using the terminology that allows our understanding to progress. Start using the terms acute coronary occlusion and occlusion MI.
Second, consider learning more about ECG in OMI, especially about features other than ST elevation that help to diagnose OMI. Learn the full progression of ECG findings of occlusion and reperfusion that have been hidden from your education due to the STEMI paradigm. Follow up your patient's cath results to learn which were false-positives or missed occlusions.
Most importantly, while waiting for the paradigm to evolve, maintain focus on our true goal for our patients with ACS: to identify and reperfuse patients with acute occlusion MI.”
That’s exactly what happened in this case. This case is part of an ongoing quality improvement initiative aimed at teaching OMI locally to emergency physicians. As a result, Dr. Cho was not distracted by the lack of STEMI criteria or the ‘old infarct’ and specially cited concerns of a subtle occlusion. The cardiologists also looked beyond STEMI criteria at the combination of clinical/ECG/echo findings to make the reperfusion decision. Had they instead followed STEMI guidelines, this patient with two STEMI negative ECGs and an initial troponin of only 100 ng/L would have been admitted as “non-STEMI” and had a worse outcome. Instead, this patient with a 100% acute coronary occlusion and a massive infarct had early intervention despite no ECG ever meeting STEMI criteria. The only problem is that the discharge diagnosis of “STEMI” obscures this fact, and perpetuates the old paradigm.
This case also shows that OMI ECG signs can be taught, both to individual and to AI. I sent
the old and new ECG from this patient to my resident Mazen, without any
information, and he replied, “I think there is proximal LAD OMI signs with
anterolateral STEs and inferior STDs.” I also sent the first ECG to the
PMcardio AI, which predicted OMI with high confidence:

PM Cardio AI is an app that:
1) takes any image of an ECG and converts it to the appropriate digital signals for AI deep neural network processing, then
2) analyzes the ECG for OMI
It was trained by Drs. Smith and Meyers
You can sign up to receive the app at this location: You can get this AI app here: https://share-eu1.hsforms.com/18cAH0ZK0RoiVG3RjC5dYdwfyfsg
Take home
1. Q waves can be acute.
2. STEMI criteria are poorly sensitive to Occlusion MI, but looking beyond ST segment elevation – including acute Q waves, and reciprocal ST depression, can help make the diagnosis.
3. Using the OMI terminology can help improve ECG interpretation and advocate for patients with STEMI(-)OMI.
4. OMI ECG signs can be learned and taught – to individuals, groups, and AI.
- The “good news” from today's case — is that Cardiology did proceed with cardiac catheterization after OMI confirmation by the rising tropoinin and bedside Echo revealing the anterior regional wall motion abnormality.
- That said — there is lots to learn from today's case as to why this patient's ongoing acute OMI should have merited cardiac catheterization sooner.
- Although millimeter criteria for a STEMI are not satisfied in ECG #1 — there are abnormal ECG findings in at least 10/12 leads!
- There is slight-but-real ST elevation in lead V2. More important — the completely straightened ST segment takeoff, with T wave volume disproportionate to QRS amplitude in this lead clearly has a hyperacute appearance in this patient with severe new chest pain.
- While I might not be certain that the ST-T wave in lead V2 is acute from this lead alone — the subtle-but-real coved ST elevation in lead aVL, in association with T wave inversion in this lead — tells us that the abnormal ST-T wave appearance in lead V2 has to be considered acute until proven otherwise.
- In further support of the acute ST-T wave abnormalities in leads aVL and V2 — is the shelf-like reciprocal ST depression in each of the inferior leads (which is especially marked in leads II and aVF).
- Continuing in this context — the coved ST elevation in lead V1 is distinctly abnormal (It's rare for there to normally be this amount of coved ST elevation in lead V1).
- This leads us to neighboring lead V3 — which instead of the gently upsloping ST segment that should be seen in this lead — there is definite straightening of the lead V3 ST segment takeoff.
- ST segment flattening with slight depression is seen in lateral leads V5 and V6, and to a lesser extent in lead I.
- Finally — a component of subendocardial ischemia is suggested by ST elevation in lead aVR that is occurring in association with the above 6 leads showing ST depression.
- PEARL: In a patient with new chest pain — Once you identify a couple of leads showing definite acute ST-T wave abnormalities (in this case — leads V2, aVL and II,III,aVF) — the more other leads you can identify showing less marked but still abnormal ST-T wave findings — the greater the chance that the ECG truly represents an ongoing acute event. At least 10/12 leads in ECG #1 show potentially acute ST-T wave changes.
- In the initial ECG — More than just a "Q" wave in lead V2 — there is a fragmented QrS complex, in which the r wave barely makes it back to the baseline. To Emphasize: This triphasic QrS appearance in lead V2 (especially given how wide the initial Q wave is) — is definite indication of "scar" from infarction at some point in time.
- It is of interest that when a prior ECG on today's patient was found (ie, ECG #2 in Figure-1) — it showed small and narrow initial q waves in leads V2-thru-V6. Normal septal q waves are generally not seen before lead V4 — though given the surprisingly tall R waves beginning with lead V2 in ECG #2 — it is likely that these small and narrow q waves in leads V2-thru-V6 of this prior tracing were not clinically significant. This confirms Dr. McLaren's point that the Q wave in lead V2 of ECG #1 is new!
- Note in ECG #1 — that although the Q wave in lead V3 is narrow, and followed by a narrow Q in lead V4 — there is no Q wave in either lead V5 or V6. Since "normal septal q waves" do not occur in leads V3,V4 without also being seen in lateral leads V5,V6 — this tells us that these Q waves in leads V3 and V4 of ECG #1 are also new.
- Finally — the Q wave in lead aVL of ECG #1 is disproportionately wide (considering QRS amplitude in this lead) — as well as being much larger than the tiny Q that was seen in lead aVL of the prior tracing.
- Not only are there new Q waves in leads V2,V3,V4 of ECG #1 — but there has been significant loss of anterior forces (ie, The surprisingly tall R waves in leads V2,V3 of the prior tracing are markedly smaller in ECG #1).
- Appreciation of the abnormal ST segment straightening in leads V2,V3 of ECG #1 — is highlighted by the change from the normal gentle ST segment upsloping that was seen on the prior tracing.
- The shelf-like ST depression seen in the inferior leads of ECG #1 is that much more remarkable as an acute change — considering that there was actually some ST elevation in the inferior leads of the prior tracing.
-USE.png) |
| Figure-1: Comparison between the first 3 tracings shown in today's case. (To improve visualization — I've digitized the original ECG using PMcardio). |
- Cardiology repeated the initial ECG in today's case — but apparently failed to consider (or at least to write down) — whether CP (Chest Pain) was still present at the time ECG #3 was recorded (and if CP was still present — was it more, less or the same as at the time ECG #1 was done?).
- Correlation of the presence and relative severity of CP at the time each serial ECG is recorded is critical — because when you compare ECG #1 with the repeat ECG ( = ECG #3 in Figure-1) — there are "dynamic" ECG changes (ie, less ST depression in the inferior leads and in leads V5,V6 of ECG #3 — and — a less acute appearance of the ST segments in leads V2,V3 of ECG #3 — and — beginning T wave inversion in leads V1,V2 of ECG #3).
- KEY Point: IF the above ST-T wave changes in ECG #3 correspond to a decrease or resolution of CP at the time ECG #3 was recorded — this would strongly suggest spontaneous reperfusion (ie, reopening of the "culprit" vessel). This would fit perfectly with the pathophysiology of ongoing coronary occlusion — and further confirms the diagnosis of an evolving acute OMI.
- BOTTOM Line: The decision by Cardiology to cath the patient in today's case was apparently not made until the 1st troponin came back elevated and bedside Echo revealed a regional wall motion abnormality. We are not told when the repeat ECG was done — but even if Cardiology failed to accept the ECG findings from the initial tracing compared to the prior tracing — a repeat ECG done no more than 15 minutes after ECG #1 and correlated with serial chest pain severity assessment — could have solidified definitive indication for cardiac cath that much sooner.
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.