
Submitted by Maura Corbett, PA-C, written by Alex Bracey, with some comments by Smith and Meyers
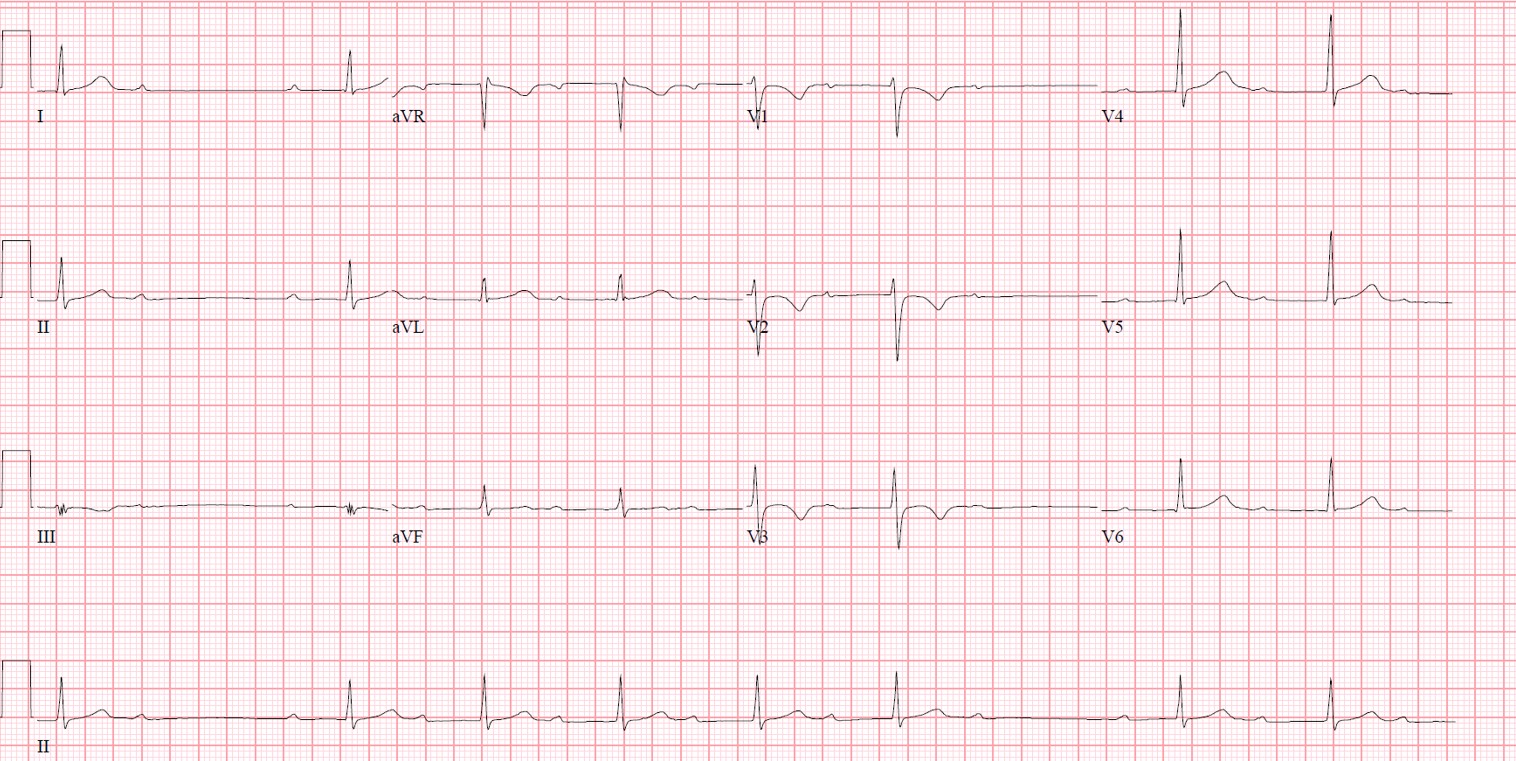
A teenage male presented to the emergency department with the complaint of dizziness with near-syncope. He was stable and able to provide a history and mentioned that he was asymptomatic while seated but dizzy and weak when attempting to stand. An ECG was performed:

{kind=link}
There is complete (third degree) heart block with wide complex bradycardic escape. The morphology is that of LBBB and so the escape is originating from the right bundle.
The possible etiologies of this ECG are:
- Structural/congenital heart disease
- Wolff-Parkinson-White
- Drug toxicity
- Myocarditis
- Infection resulting in conduction aberrancy (e.g., Lyme, rheumatic heart disease)
- Hyperkalemia
- Occlusion Myocardial Infarction (OMI)
- Pacemaker dysfunction
In this case, what is the likeliest cause of this conduction abnormality?
The answer is Lyme disease causing Lyme carditis.
(I texted the ECG to Dr. Smith with only the information that it was an adolescent patient to which he responded: "Lyme.")
This patient was seen in an emergency department in the Northeast, in which Lyme disease is endemic. Lyme disease itself is caused by the spirochete Borrelia burgdorferi and is transmitted through the Ixodes tick. Initial stages of Lyme disease have cutaneous manifestations, with later stage illness having systemic manifestations including cardiac. Lyme carditis occurs when the spirochetes directly infect cardiac tissue. Importantly, the infection can be anywhere in the cardiac tissue, including anywhere in the conduction system. In this case, the infection included the conduction system below the AV node resulting in a left bundle branch block pattern. 0.3-10% of untreated Lyme disease cases develop Lyme carditis, and 1% develop 2nd or 3rd degree AV block. AV blockade is the most common manifestation of Lyme carditis.[1,2]
For an excellent and detailed complete review on Lyme carditis check out this article by Yeung and Baranchuk:
Yeung C, Baranchuk A. Diagnosis and Treatment of Lyme Carditis: JACC Review Topic of the Week. J Am Coll Cardiol. 2019;73(6):717-726.
Lyme titers were drawn and the patient was started on ceftriaxone. He was admitted to the PICU where the following ECGs were taken in subsequent days:
Hospital Day 1
Hospital Day 1
 |
| Narrow QRS with 2nd degree AV block, type 1 Juvenile T wave inversions in anterior leads |
Hospital Day 2
 |
| Resolution of 2nd degree AV block to first degree AV block |
Hospital Day 3
 |
| Further normalizing of the conduction system with shortening of the PR interval The cardiology team was initially considering implanted pacemaker/defibrillator placement, but the patient improved with antibiotic therapy and was able to be discharged to home after an uncomplicated hospital course. His Lyme IgM was positive just prior to discharge. Teaching Points: - Consider Lyme disease as a cause of conduction abnormalities in endemic areas or with a history of recent travel to endemic areas, especially in the summer - Lyme carditis can affect any portion of the cardiac conduction system, or other cardiac tissue |
[1] Forrester JD, Mead P. Third-degree heart block associated with lyme carditis: review of published cases. Clin Infect Dis. 2014;59(7):996-1000.
[2] Yeung C, Baranchuk A. Diagnosis and Treatment of Lyme Carditis: JACC Review Topic of the Week. J Am Coll Cardiol. 2019;73(6):717-726.
very interesting indeed. thank you all.
ReplyDelete