
This case was written by Andy Lichtenheld (https://twitter.com/ALichtenheld), a really smart 2nd year resident here at our Emergency Medicine program at Hennepin County Medical Center.
Here is some shameless promotion of our residency, which was started in 1972 and which we think is second to none:
Here is some shameless promotion of our residency, which was started in 1972 and which we think is second to none:
Learn why our current residents chose Hennepin.
Case
A 70-something woman with a history of CAD arrived by EMS after a syncopal episode. She had been in her usual state of health when she suddenly became lightheaded and collapsed. She regained consciousness prior to EMS arrival and arrived in the ED confused but gradually clearing. She had no chest discomfort, shortness of breath, arm pain, jaw pain or any other symptoms.
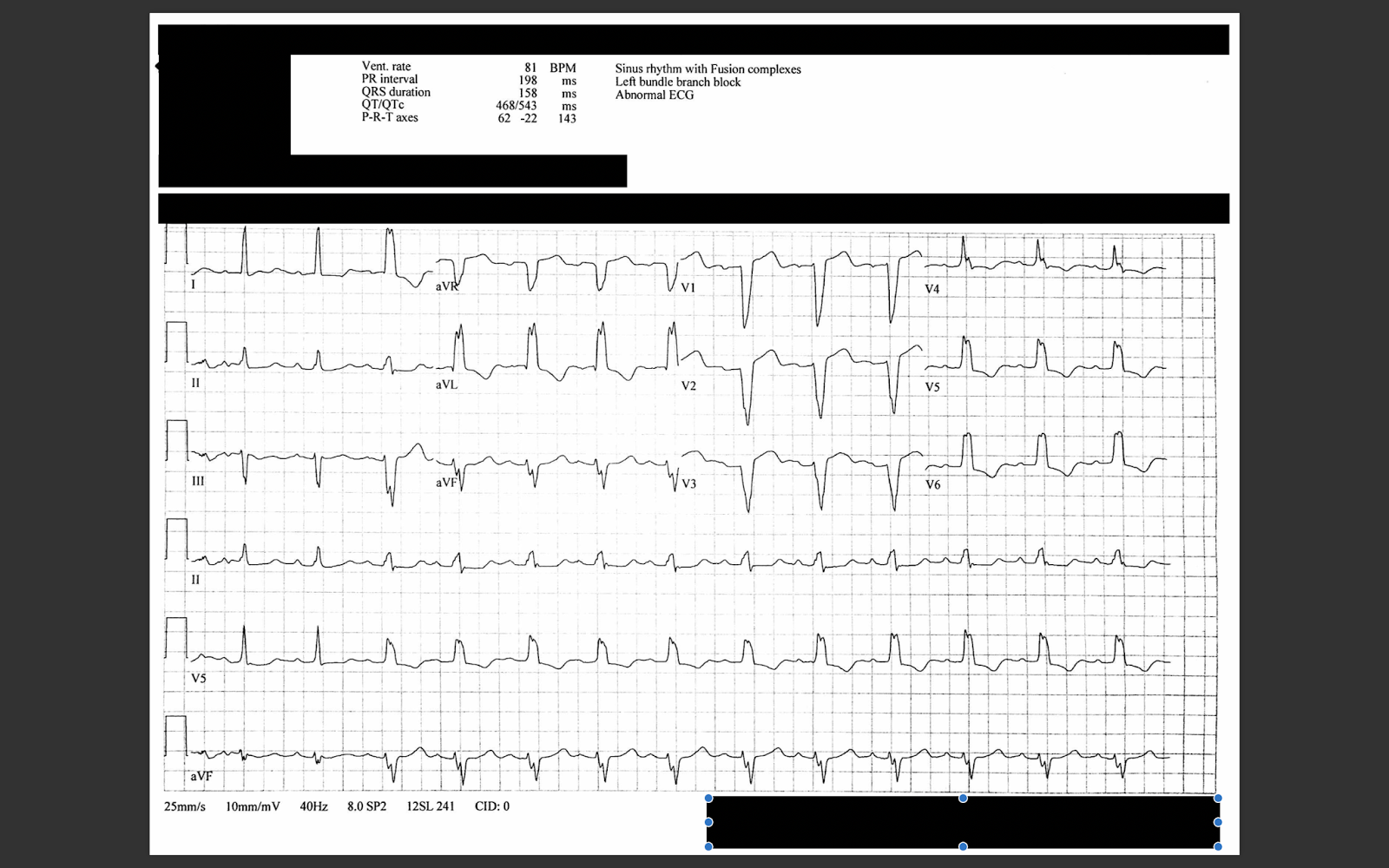
An initial ECG was recorded:
 |
| What do you think? |
The computer has identified it as sinus with a Mobitz I AV block with a LBBB.
However, both the rhythm and QRST appear to be more complicated.
Rhythm: Regular P-waves can be seen throughout the rhythm strip. Without using calipers and without using more thought than necessary in an emergency, it is hard to say whether this is first or second degree AV block with conduction to a left bundle branch block, or if it is third degree (complete) heart block with an escape from the right ventricle. Beats 3 and 5 are PVCs.
Smith: After scrutinizing at leisure, I do think it is complete heart block with an RV escape, but it is complicated.
What else?
There is excessively discordant ST elevation in V1 & V2. ST/S ratio in V1 is 5/15 = 33%.
There is excessively discordant ST elevation in aVR. The ST/S ratio is 3/8 = 37%.
There is also excessively discordant ST depression in lead I (ST/R ratio = 100%) and V4 (ST/R ratio = ~60%).
If you accept, as Dr. Smith does, that the Smith Modified Sgarbossa criteria can be used not only in LBBB, but also in ventricular escape rhythms, then any one of these findings meets those criteria. The STE in V1 as well as the STD in I and V4 are particularly specific for occlusion.
Furthermore, there is an abnormal amount of STD in V5 and V6 (ST/R ratio almost 20%).
Smith Modified Sgarbossa Criteria for LBBB and Ventricular Paced Rhythms
Rule 1: (80-90% sensitive, 95% specific for occlusion)
Any one of:
1. 1 mm concordant STE in any one lead
2. 1 mm concordant STD in any one of V1-V3
3. At least 1 mm discordant STE that is ≥25% of the preceding S-wave in at least one lead
Rule 2: (Only 64% sensitive, but 98% specific for occlusion)
Any one lead with proportionally discordant STE or STD of at least 30% of the preceding R- or S-wave
Smith comment:
One more finding!! PVCs!!!! The 5th beat is a PVC and has an RBBB morphology (large R-wave in aVR with wide S-wave in V5). This implies a PVC originating in the left ventricle. RBBB morphology PVCs should never have an ST segment that is concordant to the QRS, as it is here in lead aVR. This is diagnostic for STEMI.
See these cases:
Case continued
A previous ECG was obtained:
 |
There is a preexisting LBBB with proportionally normal discordant ST elevation, which makes the ST changes in the new EKG obvious by comparison.
This also suggests that the rhythm in the first ECG is supraventricular, because the QRS morphology is LBBB. However, if you look closely at V5 and V6 in the first ECG, both have a very narrow peak compared to this old ECG which is much more typical LBBB.
|
Smith comment: I am still not completely certain as to whether the first ECG is supraventricular with left bundle branch block, or with RV escape. But it does not matter: the patient has a coronary occlusion until proven otherwise. She needs immediate pacer pad placement and angiography/PCI.
Case Continued
The clinicians caring for the patient were concerned about an acute coronary occlusion. The cardiologist was in hospital and was paged to the resuscitation area. Over the course of the following few minutes, the patient gradually recovered to her normal mental status. She remained normotensive and entirely asymptomatic.
As the cardiologist arrived, a change in the QRS morphology was noted on the monitor and a repeat ECG was obtained:
 |
| What is your interpretation? |
Now there is definitely complete heart block with a ventricular escape:
--The predominant QRS morphology is now RBBB + LAFB with interposed PVC's, which indicates a dominant escape focus now in the left posterior fascicle.
--The ST elevation in V1 and V2 with reciprocal ST depression are now obvious. It is RBBB morphology with ST elevation concordant to the R-wave, similar to the PVC mentioned above. This does not happen without ischemia.
--There is marked ST depression in lead II which is then attenuated in aVF and then entirely absent in lead III.
Smith comment: What is the infarct artery??? With STE in V1 and aVR, one might think this is LAD or left main. Such a conclusion would be consistent with the diffuse ST depression.
The ST axis is exactly towards aVR, which is what you expect with diffuse subendocardial ischemia (ST depression vector towards I and II, with a reciprocal ST elevation vector towards aVR). However, the ST elevation is so much more pronounced than the ST depression.
Is there something else going on??
Andy Lichtenheld wrote: "This is also consistent with inferior and large RV MI due to proximal RCA occlusion."
Case continued:
The initial troponin I returned elevated at 4.5 ng/mL.
She was taken to the cath lab where a 90% proximal RCA lesion, proximal to the RV marginal branch, was stented and a temporary pacemaker was placed.
The next day echo showed very poor LV function with an inferior wall motion abnormality.
Smith comment:
So Dr. Lichtenheld was correct. It was an inferior + right ventricular (RV) STEMI.
This pattern of ST elevation and depression is often due to LAD or left main.
I can't fully explain why there was no ST elevation in the inferior leads, especially lead III.
See this case:
Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6
More on ECG in inferior and RV MI:
http://hqmeded-ecg.blogspot.
Here are comments from Ken Grauer:
Fascinating case, about which we’ll probably never know the mechanism of the rhythms for certain. I’ll make a few speculations. I suspect that ECG #1 was not complete AV block — because of the clear irregularity of the ventricular response. In most cases with complete AV block — the ventricular response will be more regular. We see this in ECG #3, in which there clearly IS complete AV block. Returning to ECG #1 — the atrial rhythm is NOT regular. Initially P waves are buried within the ST segment of the first few beats. If you follow out atrial deflections carefully with calipers — the P-P interval varies in a difficult-to-predict manner in some parts of the parts of the tracing. This can happen with atrial infarction, though we really do not see P wave ST segment deviation … QRS morphology in ECG #1 I believe is consistent with LBBB (albeit with lots of fragmentation) — with beats #3 and #5 being PVCs. As per Dr. Smith — the situation is extremely complex. I suspect there may be atypical Wenckebach (PR intervals increasing to quite long toward the end of the tracing) — though R-R interval periodicity is clearly atypical. What IS apparent (as per Dr. Smith) — is that ST-T wave morphology that we see in ECG #1 is abnormal regardless of the etiology of the QRS complex. This ST-T wave abnormality in ECG #1 was confirmed when the baseline LBBB tracing was obtained. NOTE — The first 2 beats in ECG #2 conduct with a NARROW QRS complex — which suggests that this patient’s “baseline” ECG had a rate-related LBBB! I believe that theory is confirmed in ECG #3, which as per Dr. Smith now definitely DOES show complete AV block — with regular escape rhythm and now clearly much more regular atrial activity than we saw in ECG #1. I believe we may have an AV nodal (junctional) escape rhythm in ECG #3 — as the escape rate is ~50/minute, and QRS morphology looks VERY supraventricular given well definite RBBB-morphology in anterior leads and sharp/narrow initial deflections in lateral leads with wide terminal S waves. The heart rate is slower — so the rate-related LBBB has now resolved. We are left with a pattern of marked ST elevation in V1,V2,V3 — with maximal ST elevation in lead V1. As astutely pointed out by Dr. Lichtenheld — this pattern is consistent with isolated acute RV infarction! Of note — virtually all other leads on ECG #3 show significant scooped ST depression (actually a “mirror-image” shape opposite to the coved ST elevation in V1,V2,V3 — so my thought is that in addition to acute RV infarction — there was diffuse subendocardial ischemia. Note however, that there IS suggestion of ST coving in lead III on ECG #3, as well as relatively LESS ST depression in lead aVF — so perhaps the reason we did not see ST elevation in the inferior leads, is that this was essentially cancelled out by the diffuse subendocardial ischemia ST depression seen in virtually all other leads except V1,2,3? Finally — If we go back to ECG #1 (when there was rate-related BBB) — we actually DO see the same type of ST segment deviations that we see in ECG #3 — with the difference being that these ST deviations in ECG #1 were partially masked by the underlying rate-related LBBB. That is, marked ST coving in lead III, ST elevation in V1,2,3 — and dramatic ST depression (beyond the amount expected for LBBB) in all other leads. GREAT case! Thanks for presenting!
Here are comments from Ken Grauer:
ECG Interpretation
Fascinating case, about which we’ll probably never know the mechanism of the rhythms for certain. I’ll make a few speculations. I suspect that ECG #1 was not complete AV block — because of the clear irregularity of the ventricular response. In most cases with complete AV block — the ventricular response will be more regular. We see this in ECG #3, in which there clearly IS complete AV block. Returning to ECG #1 — the atrial rhythm is NOT regular. Initially P waves are buried within the ST segment of the first few beats. If you follow out atrial deflections carefully with calipers — the P-P interval varies in a difficult-to-predict manner in some parts of the parts of the tracing. This can happen with atrial infarction, though we really do not see P wave ST segment deviation … QRS morphology in ECG #1 I believe is consistent with LBBB (albeit with lots of fragmentation) — with beats #3 and #5 being PVCs. As per Dr. Smith — the situation is extremely complex. I suspect there may be atypical Wenckebach (PR intervals increasing to quite long toward the end of the tracing) — though R-R interval periodicity is clearly atypical. What IS apparent (as per Dr. Smith) — is that ST-T wave morphology that we see in ECG #1 is abnormal regardless of the etiology of the QRS complex. This ST-T wave abnormality in ECG #1 was confirmed when the baseline LBBB tracing was obtained. NOTE — The first 2 beats in ECG #2 conduct with a NARROW QRS complex — which suggests that this patient’s “baseline” ECG had a rate-related LBBB! I believe that theory is confirmed in ECG #3, which as per Dr. Smith now definitely DOES show complete AV block — with regular escape rhythm and now clearly much more regular atrial activity than we saw in ECG #1. I believe we may have an AV nodal (junctional) escape rhythm in ECG #3 — as the escape rate is ~50/minute, and QRS morphology looks VERY supraventricular given well definite RBBB-morphology in anterior leads and sharp/narrow initial deflections in lateral leads with wide terminal S waves. The heart rate is slower — so the rate-related LBBB has now resolved. We are left with a pattern of marked ST elevation in V1,V2,V3 — with maximal ST elevation in lead V1. As astutely pointed out by Dr. Lichtenheld — this pattern is consistent with isolated acute RV infarction! Of note — virtually all other leads on ECG #3 show significant scooped ST depression (actually a “mirror-image” shape opposite to the coved ST elevation in V1,V2,V3 — so my thought is that in addition to acute RV infarction — there was diffuse subendocardial ischemia. Note however, that there IS suggestion of ST coving in lead III on ECG #3, as well as relatively LESS ST depression in lead aVF — so perhaps the reason we did not see ST elevation in the inferior leads, is that this was essentially cancelled out by the diffuse subendocardial ischemia ST depression seen in virtually all other leads except V1,2,3? Finally — If we go back to ECG #1 (when there was rate-related BBB) — we actually DO see the same type of ST segment deviations that we see in ECG #3 — with the difference being that these ST deviations in ECG #1 were partially masked by the underlying rate-related LBBB. That is, marked ST coving in lead III, ST elevation in V1,2,3 — and dramatic ST depression (beyond the amount expected for LBBB) in all other leads. GREAT case! Thanks for presenting!
No comments:
Post a Comment
DEAR READER: I have loved receiving your comments, but I am no longer able to moderate them. Since the vast majority are SPAM, I need to moderate them all. Therefore, comments will rarely be published any more. So Sorry.