
An elderly man with a history of diabetes and HTN presented with lethargy and weakness, decreased urine output, and hypotension. There was no history of any GI bleeding or other hemorrhage. There was no fever.
He had no CP or SOB, and it was unknown if there was a previous history of atrial fib. He was on atenolol, but it was not known if this was simply for hypertension, or for atrial fib.
He was not anti coagulated.
Blood pressures ranged from 83/45 to 125/83, lower than usual. HR ranged from 110 to 145.
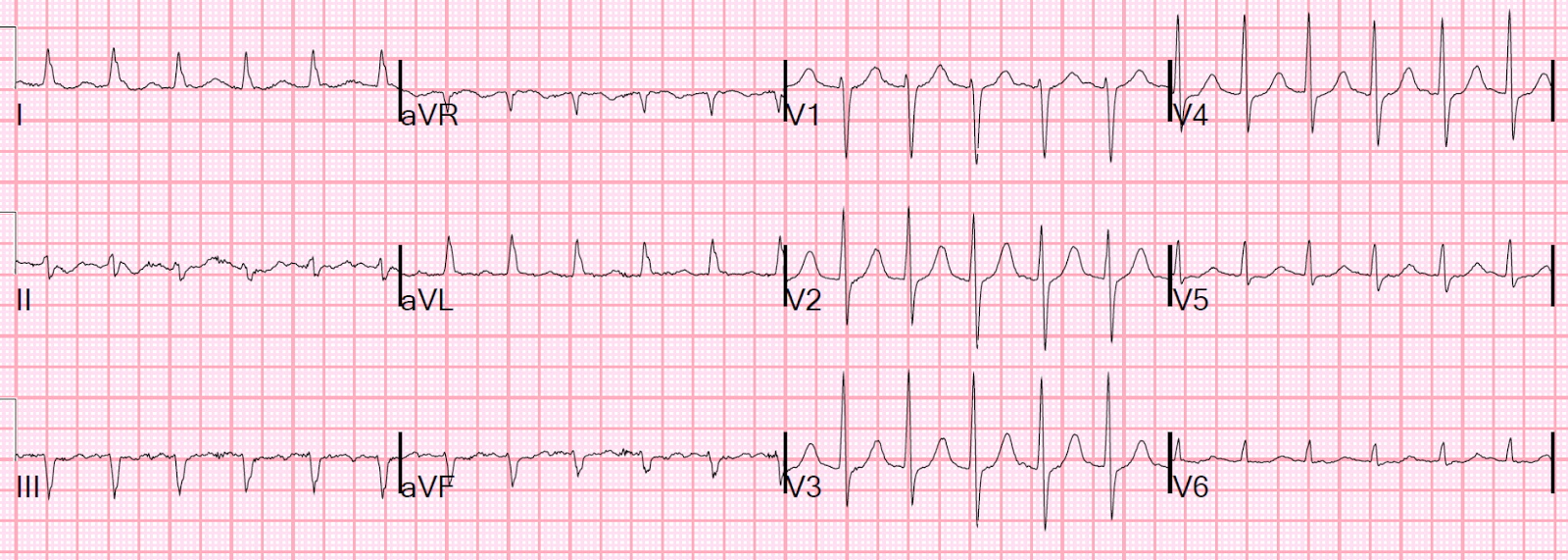
He had an ECG recorded upon arrival:
The ischemia on the ECG could be of several possible etiologies:
1) New atrial fib with RVR causing demand ischemia (but the rate is not terribly fast).
2) Old atrial fib with poor rate control causing demand ischemia.
3) ACS with possible additional ischemia from atrial fib with RVR
4) Hemorrhage/dehydration/sepsis/etc., with new or old atrial fib, resulting in reflexive tachycardia and demand ischemia.
To find the answer, it is wise to assess volume status, which can be done with ultrasound:
A bedside ultrasound was done from the subcostal view, concentrating on the IVC. If this is due to etiologies 1-3, one would expect a full IVC. If etiology 4, then one expects a flat and/or collapsing IVC:
This shows a collapsing inferior vena cava (IVC), consistent with volume depletion
Another with a better view of the heart. RV is on upper part of the view, next the liver:
RV is quite small. LV is also small and has good contractility. This supports volume depletion.
The appropriate therapy would be fluids and further workup for hemorrhage/dehydration/sepsis/etc.
However, BOTH an esmolol bolus and drip, and IV fluids were started.
But beta blockade should NOT be given, at least not yet. In a volume depleted state, this patient needs the reflexive tachycardia for cardiac output.
By the time I arrived and was involved, the esmolol had not been at a high enough dose to do any harm.
His lactate returned as 3.3 mEq/L and first troponin at 0.139 ng/mL. I was quite certain that this was a type II (demand ischemia) MI and that this patient was not having ACS.
I assume that cardioversion was appropriately not done because the risk of thromboembolism, but other reasons not to do it are: 2) if the patient is in chronic atrial fib, it is unlikely to work and 3) the etiology of mild shock is NOT the atrial fib with RVR, but some other illness that can be at least partly alleviated with IV fluids.
I stopped the esmolol and gave the patient 2 liters of fluid. After fluids, the IVC was less collapsing:
The volume status is now better, at least relatively. It still may not be enough: when patients are in atrial fib, they usually need higher filling pressures for good cardiac output, so some IVC fullness would be good, as long as it does not lead to pulmonary edema, best evaluated with B-lines.
There were no B-lines.
But the patient monitor then showed a regular tachycardia without any P-waves. The rate was very constant at 140 and so I wondered if this was SVT or sinus tach. Another ECG was recorded:
I went into the patient's room, and, according to the interview with Christopher Watford on EMCrit, I changed the monitor leads around (this is not a 12-lead!)
So the patient now has sinus tachycardia.
I gave more fluids and the heart rate came down. Here is the next ECG:
Later, the second troponin I returned at 0.562 ng/mL. When the third returned, it was 2.165 ng/mL.
He developed a fever and urine showed WBC's. He was treated for urosepsis and did well. He did not have ACS.
Learning Points:
1. Not all myocardial infarction is due to ACS
2. Atrial fibrillation with RVR may be a consequence, not a cause of, illness
3. Volume status is critical in the management of Atrial fibrillation with RVR
4. If you are not certain of a source of SVT, do Lewis leads
He had no CP or SOB, and it was unknown if there was a previous history of atrial fib. He was on atenolol, but it was not known if this was simply for hypertension, or for atrial fib.
He was not anti coagulated.
Blood pressures ranged from 83/45 to 125/83, lower than usual. HR ranged from 110 to 145.
He had an ECG recorded upon arrival:
 |
| There is atrial fibrillation with a rapid ventricular response (rate of approximately 120). There are aberrantly conducted beats (Ashmann's phenomenon), which are easily confused with runs of VT. There is ST depression in V2-V6 that is clearly ischemic. |
1) New atrial fib with RVR causing demand ischemia (but the rate is not terribly fast).
2) Old atrial fib with poor rate control causing demand ischemia.
3) ACS with possible additional ischemia from atrial fib with RVR
4) Hemorrhage/dehydration/sepsis/etc., with new or old atrial fib, resulting in reflexive tachycardia and demand ischemia.
To find the answer, it is wise to assess volume status, which can be done with ultrasound:
A bedside ultrasound was done from the subcostal view, concentrating on the IVC. If this is due to etiologies 1-3, one would expect a full IVC. If etiology 4, then one expects a flat and/or collapsing IVC:
This shows a collapsing inferior vena cava (IVC), consistent with volume depletion
Another with a better view of the heart. RV is on upper part of the view, next the liver:
RV is quite small. LV is also small and has good contractility. This supports volume depletion.
The appropriate therapy would be fluids and further workup for hemorrhage/dehydration/sepsis/etc.
However, BOTH an esmolol bolus and drip, and IV fluids were started.
But beta blockade should NOT be given, at least not yet. In a volume depleted state, this patient needs the reflexive tachycardia for cardiac output.
By the time I arrived and was involved, the esmolol had not been at a high enough dose to do any harm.
His lactate returned as 3.3 mEq/L and first troponin at 0.139 ng/mL. I was quite certain that this was a type II (demand ischemia) MI and that this patient was not having ACS.
I assume that cardioversion was appropriately not done because the risk of thromboembolism, but other reasons not to do it are: 2) if the patient is in chronic atrial fib, it is unlikely to work and 3) the etiology of mild shock is NOT the atrial fib with RVR, but some other illness that can be at least partly alleviated with IV fluids.
I stopped the esmolol and gave the patient 2 liters of fluid. After fluids, the IVC was less collapsing:
The volume status is now better, at least relatively. It still may not be enough: when patients are in atrial fib, they usually need higher filling pressures for good cardiac output, so some IVC fullness would be good, as long as it does not lead to pulmonary edema, best evaluated with B-lines.
There were no B-lines.
But the patient monitor then showed a regular tachycardia without any P-waves. The rate was very constant at 140 and so I wondered if this was SVT or sinus tach. Another ECG was recorded:
 |
| Now there is a regular supraventricular rhythm. There are probable P-waves, but I wasn't entirely certain. What to do? Lewis Leads. |
I went into the patient's room, and, according to the interview with Christopher Watford on EMCrit, I changed the monitor leads around (this is not a 12-lead!)
- Place the Right Arm electrode on the patient’s manubrium.
- Place the Left Arm electrode on the 5th intercostal space, right sternal border.
- Place the Left Leg electrode on the right lower costal margin.
- Monitor Lead I.
I printed it out. This is what I recorded:
| Now the P-waves are obvious |
So the patient now has sinus tachycardia.
I gave more fluids and the heart rate came down. Here is the next ECG:
 |
| Normal |
Later, the second troponin I returned at 0.562 ng/mL. When the third returned, it was 2.165 ng/mL.
He developed a fever and urine showed WBC's. He was treated for urosepsis and did well. He did not have ACS.
Learning Points:
1. Not all myocardial infarction is due to ACS
2. Atrial fibrillation with RVR may be a consequence, not a cause of, illness
3. Volume status is critical in the management of Atrial fibrillation with RVR
4. If you are not certain of a source of SVT, do Lewis leads
Hi Dr Smith, his scenario is actually relatively common. If the source of infection is obvious and septic shock is a real concern, would you consider a norepinephrine drip early, despite fluid loading and the patient remaining hypotensive with AF and RVR?
ReplyDeleteI'm thinking if the flat IVC is due to venoplegia, then vasopressors might work and the AF and RVR might actually slow down. On the other hand, may not because of beta 1 efffects.
Thanks,
That's a tough question that is not fully resolved in sepsis literature, as far as I can tell. Lots of controversy about when to stop fluids and start pressors. I think if you can give fluids to the point where you're not causing pulmonary edema, then you're ok doing that. But where is that point? Once you have B-lines, there is pulmonary edema, but it might be quite mild and managable as long as there are no other signs of pulmonary edema (e.g., CXR, SOB, rales).
DeleteSteve Smith
It is known that the mean P wave axis is between +30 to +75 degree ...
ReplyDeleteAnd i think that lewis lead is arrangement is about +90 degrees in space SO why it is best for detecting atrial Ps .... it is not so parrallel to it's axis ???
good question. I'm going to refer you to references:
Deletehttp://circ.ahajournals.org/content/119/24/e592
https://emcrit.org/wp-content/uploads/2011/11/Lewis-Lead-Enhances-Atrial-Activity-Detection-in-Wide-QRS-Tachycardia.pdf
The regular ekg could be flutter?
ReplyDeletewe cannot rule it out
It has none of the features of flutter. Then the Lewis leads prove it is sinus.
Deleteit is interesting that some folk (paul marik, eg) say that fluids may harm, and waiting for B lines, or even a plethoric IVC may be waiting too late. some say load them up with the 30ml/kg regardless, and intubate if need be.
ReplyDeletethe latest i read was regarding US for portal vein pulsatility. all quite challenging.
steve, do you think this may be a case for considering phenylephrine push-pressor, where one may want pure vasoconstriction, without the beta, in those patients who are afib tachy, hypotensive, at least until the bp improves,
i addition to discretionary fluids.
and now , after josh farkas' post on emcrit, should those fluids be LR, or plasmalyte, and not "normal" saline.
thank you
tom
Tom,
DeleteI would frankly cardiovert electrically, unless there is evidence that this is chronic atrial fib.
I would assess IVC and, if flat, also give fluids.
I don't think there is any data other than anecdotal on push dose pressors, especially for this.
Read this: https://pdfs.semanticscholar.org/3061/fe3c41137f8918dbdf688213769fecdc863e.pdf
Steve