
A male in his early 20s presented intoxicated, with no CP or SOB. An ECG was obtained for tachycardia.
First ECG:
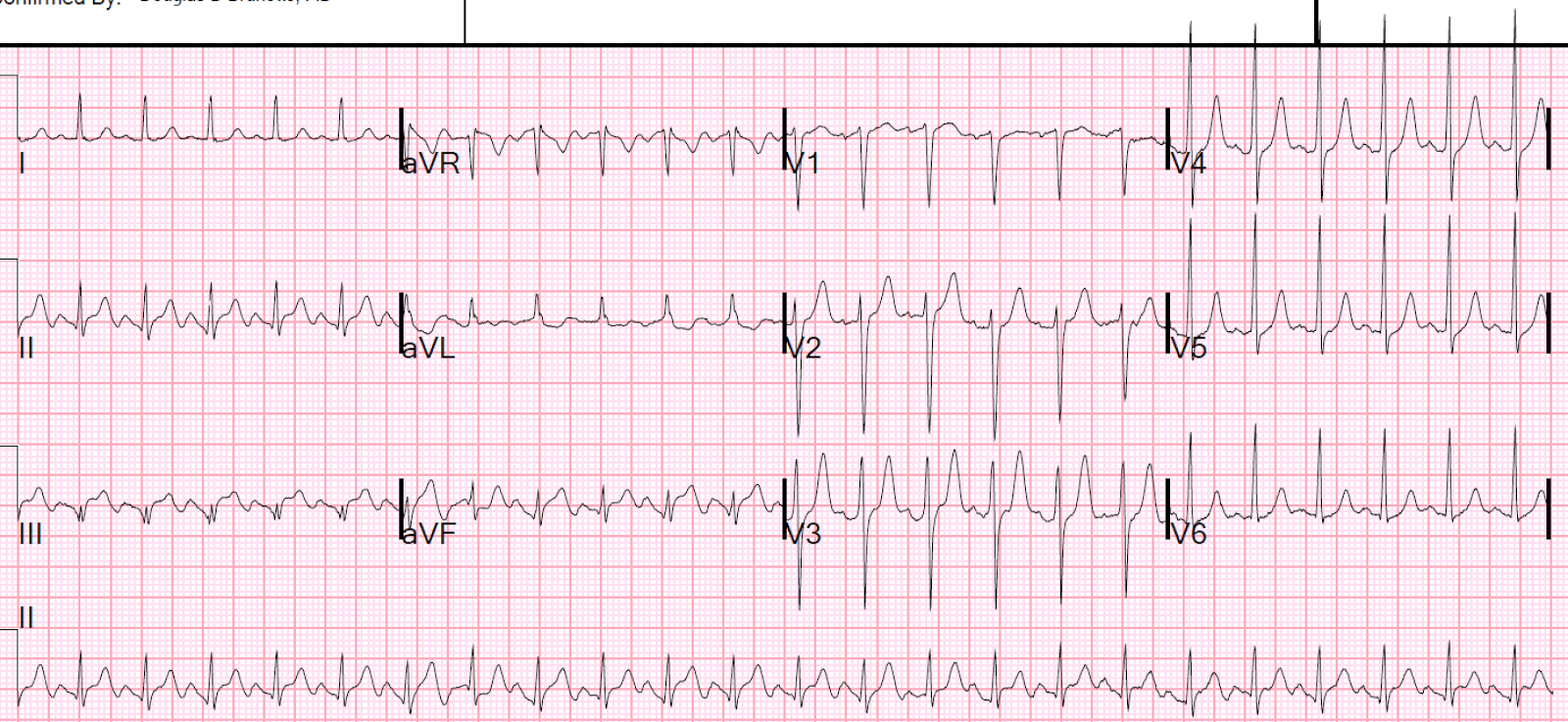 |
| Sinus tachycardia at 150. There is inferior ST Elevation and Q-waves that appear to be Inferior STEMI. There is reciprocal ST depression in aVL. Is this STEMI? |
The patient was very dehydrated.
The physicians were worried about STEMI, and so did a Point of Care Cardiac Ultrasound which showed IVC collapse and hyperdynamic function.
The patient had a previous visit with dehydration
 |
| There had been some, but less, STE Not very similar to this one. |
There was another previous visit with dehydration
 |
| Also not similar |
He was given 2 liters of IV fluids. A 2nd ECG was recorded 1 hour later:
 |
| Sinus tach at a rate of 120 Heart rate and ST segments are almost normalized |
 |
| What do you see now? See below. |
Unexpectedly, there is every other beat pre-excitation. So the patient has WPW. This was never diagnosed before. But I don't think this explains his ST segments.
Clinical course
3 serial troponins were below the 99% level of 0.030 ng/mL, but not undetectable.
K was 4.5 mEq/L.
The patient was rehydrated and discharged.
Comment:
Why the PseudoSTEMI pattern?
I don't know for certain, and this ECG sure looks like inferior STEMI. However, patients with STEMI generally do not have tachycardia unless they are in cardiogenic shock. If such is the case, the patient should have high filling pressures and high right sided pressures and NOT have a collapsed IVC. They should also not be hyperdynamic.
It is possible to be dehydrated AND have a STEMI, but in that case the best initial treatment is supportive: rehydration. Then re-evaluation.
So it was perfectly appropriate to do a bedside ultrasound and, finding a hyperdynamic heart, to defer diagnosis of ACS and give fluids. Even if this STE is due to ischemia, it is most likely due to demand ischemia, NOT due to ACS, and the best initial therapy is to hydrate. In our many studies of type 2 MI, we found that 2-5% had ST elevation on the ECG.
Final comment:
I sent this to Ken Grauer, who is a fantastic ECG resource and has much experience with stress ECGs, and asked if this is a pattern he has seen in stress tests. He stated "no," (in a few more words than that).
Fascinating case with a number of interesting insights to learn. Diagnosis of alternate preexcitation on the last tracing is subtle, but important to recognize. The 2 other thoughts I considered in my differential diagnosis for this last ECG were: i) electrical alternans; and ii) ventricular bigeminy with fusion from end-diastolic PVCs — but neither “fit” (that’s because we see DELTA waves in several leads on this tracing that provide the diagnosis). Otherwise — the T wave peaking we see on the tachycardia ECGs is extremely interesting. I have often seen T wave peaking with tachycardia (and on stress tests) in otherwise healthy young adults — but I don’t expect ST elevation. In addition, this patient was apparently markedly dehydrated on each occasion when the ECG was done. Hyperkalemia (perhaps secondary to volume contraction) not uncommonly leads to T wave peaking with recurrent episodes, but again supposedly not associated with ST elevation (Wonder what serum K+ values were in this patient with recurrent dehydration?). I guess we have to add a “pseudo-infarction pattern” to the list of ECG peculiarities that may be seen with marked sinus tachycardia. THANKS to Dr. Smith for posting this intriguing case!
ReplyDeleteK was normal
DeleteOut of interest, did he have a positive troponin?
ReplyDeleteAll negative, as stated in case.
DeleteExcellent sir
ReplyDeleteRecently I have a young severe DKA patient with STE inferolateral and completed resolved after adequate hydration in just few hours
Serial trop were all normal
Interesting thought ��
STE like that is common (inferolateral early repol), but were there Q-waves and reciprocal STD in aVL??
DeleteWhat I know abt SVT with aberrancy vs VT is that SVT should have exactly same 12 lead morphology in tachy state as in baseline.
ReplyDeleteTks..
Hello AKS. I'm not sure I understand your comment ... Aberrant conduction is often (not always) rate-related — and most often conducts in a pattern suggestive of some form of conduction block (ie, rbbb, lbbb, lahb, lphb, rbbb/lahb, rbbb/lphb). But morphologies are not "fixed" — so there may be some variation in the type of aberrant pattern you see. OTHERWISE — there is a VERY common misconception made by many folks in my experience. That is that there are 2 DIFFERENT phenomena: #1) QRS widening with an SVT because of PREEXISTING BBB (in which case YES, the QRS will look identical at fast and slow rates); and #2) Rate-related aberrant conduction — in which the QRS is narrow and normal at rest — but at some faster rate, because there isn't enough time for part of the conduction system to recover — you see a rate-related BBB morphology. I hope this clears up your question — :)
DeleteSorry Ken.
ReplyDeleteI put my comment in the wrong post.