
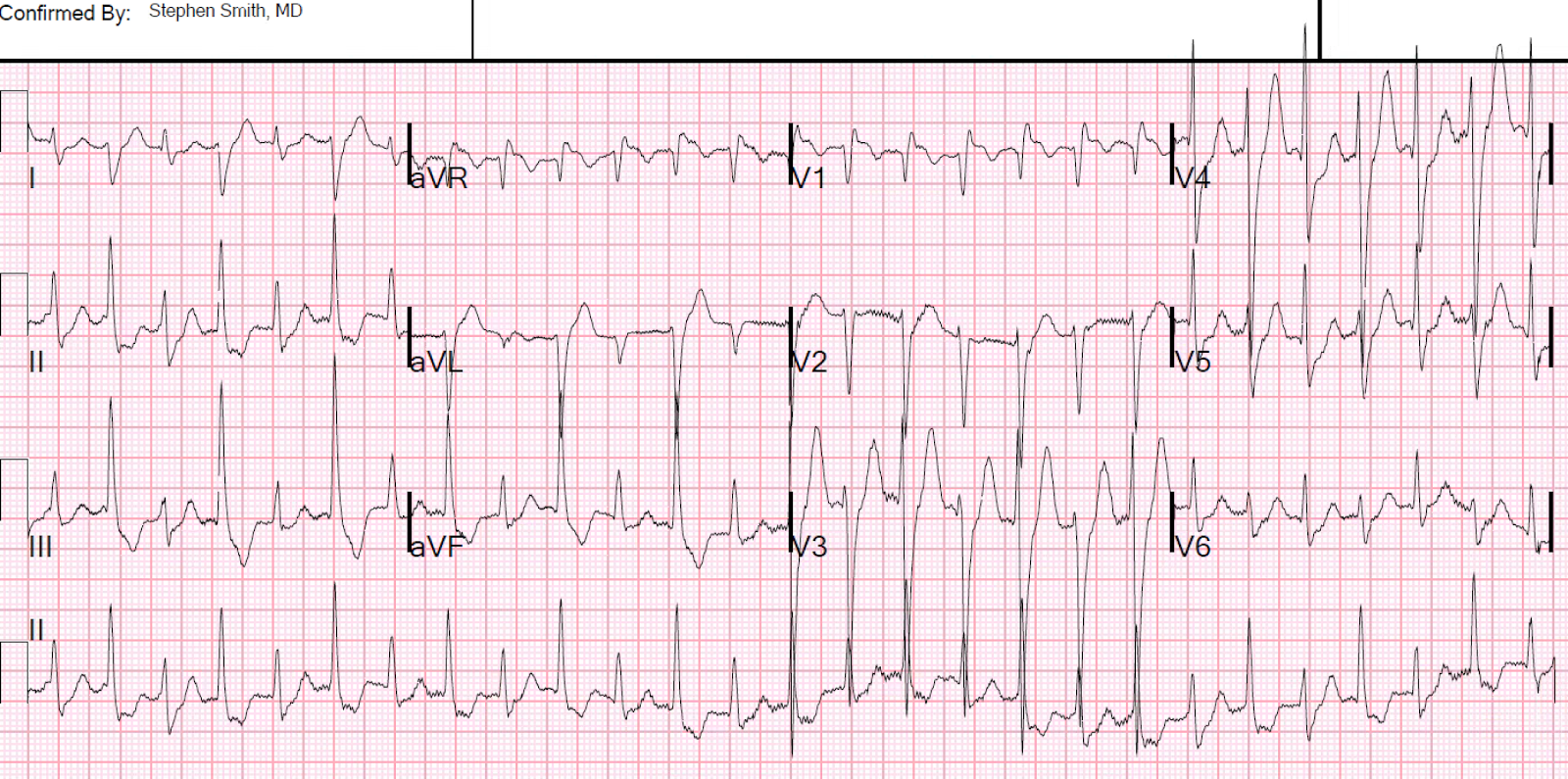
A middle aged woman with few serious medical issues presented with altered mental status, had a generalized tonic clonic seizure, and was found to be hypertensive and tachycardic. An ECG was recorded:
This is a regular, wide complex tachycardia, but not very wide. There are no P-waves. The QRS has 2 alternating morphologies, both of which are right bundle branch block (RBBB) in configuration, but which have different axes. Both complexes have an rSR' in lead V1 and a wide S-wave in V6.
One might suspect that the higher voltage beats are premature beats, but by my calipers, the intervals are identical. (This is critical to being certain that they are not premature beats.) Similarly, one might suspect every-other-beat pre-excitation, but no delta waves are seen.
See how the S-wave in lead I alternates small, large, small, large... The large S-wave indicates right axis deviation and appears to be due to alternating left posterior fascicular block, in addition to RBBB.
So this is SVT with alternating aberrancy: RBBB, then RBBB + LPFB, then RBBB, then RBBB + LPFB.....
The question of electrical alternans came up. SVT frequently has electrical alternans but, unlike in sinus tach, it is not correlated with effusion or tamponade. In this case, it is not the typical SVT electrical alternans -- the alternans is due to alternating conduction.
She spontaneously converted:
 |
| What is it? The computer measures QRS duration as 126 ms. |
This is a regular, wide complex tachycardia, but not very wide. There are no P-waves. The QRS has 2 alternating morphologies, both of which are right bundle branch block (RBBB) in configuration, but which have different axes. Both complexes have an rSR' in lead V1 and a wide S-wave in V6.
One might suspect that the higher voltage beats are premature beats, but by my calipers, the intervals are identical. (This is critical to being certain that they are not premature beats.) Similarly, one might suspect every-other-beat pre-excitation, but no delta waves are seen.
See how the S-wave in lead I alternates small, large, small, large... The large S-wave indicates right axis deviation and appears to be due to alternating left posterior fascicular block, in addition to RBBB.
So this is SVT with alternating aberrancy: RBBB, then RBBB + LPFB, then RBBB, then RBBB + LPFB.....
The question of electrical alternans came up. SVT frequently has electrical alternans but, unlike in sinus tach, it is not correlated with effusion or tamponade. In this case, it is not the typical SVT electrical alternans -- the alternans is due to alternating conduction.
She spontaneously converted:
 |
| Sinus tachycardia with normal conduction. Normal QRS, narrow, normal axis. This confirms that the SVT caused the aberrancy.
ST depression consistent with ischemia.
She was found to have a BP of 300/180, and sinus tachycardia at a rate as high as 150. This blood pressure and heart rate were successfully controlled with clevidipine and esmolol. The patient was found on MRI to have "Posterior Reversible Encephalopathy Syndrome" (PRES), which is not always posterior and not always reversible, and which formerly was called "hypertensive encephalopathy." The extreme hypertension and sinus tachycardia led to suspicion of pheochromocytoma.
The etiology of the SVT is uncertain, but is probably AVNRT that was initiated in this hyperadrenergic state. The aberrancy is due to refractoriness of the right bundle at this high rate, and a posterior fascicle which is only able to recover on every other beat, but is still refractory on the beats inbetween. The right bundle nearly always has a longer refractory period than the left bundle and aberrancy is thus much more likely to show RBBB morphology. Here is another case of SVT with alternating aberrancy An Unusual Tachycardia
Is there an alternative explanation?
Bidirectional Ventricular Tachycardia may be due to a "ping-pong" effect of alternating VT origin in the left bundle vs. right bundle. It is conceivable that this could be fascicular VT with an alternating origin in the left bundle, then left anterior fascicle, back and forth. Then it would be a bidirectional fascicular VT. I've never heard of this before and could not find any literature on it, so it probably doesn't exist and this hypothesis is pure speculation. See Ken Grauer's comments on this differential diagnosis, pasted below. As always, it is very incisive!
Ken Grauer's comments I'd bet this is alternating RBBB with RBBB/LPHB aberration. I had not heard of bidirectional fascicular VT — and I'm sure it is rare indeed. My impression from the fascicular VTs that I've seen — is that although they resemble some pattern of bifascicular block (rbbb/lahb or rbbb/lphb) — they are usually NOT as "clean" as can be the case with aberrancy or preexisting bbb. Of course, aberrancy and preexisting bbb/hemiblock patterns are not always "clean" (they may show squiggle, notches, lack that clear S wave in V1, etc) — but when you do see a bbb or bifascicular block pattern that is "clean" — my impression is that it is almost certain to be supraventricular; and not ventricular in etiology. I believe that is the case here. In some leads (like lead II) — you'll note not only the initial direction, but also the initial slope of the initial deflection is identical for both complexes. If we were switch from one site of fascicular VT to another — I would not expect to see this. In other leads — the very fine detail of the initial deflection is doing exactly as I would expect it to do if the problem was alternating LPHB with every other beat. That is, in lead I with LPHB beats — there is a tiny-but-present initial r wave — but instead there is a tiny-but-present initial q wave when we only have RBBB. And in lead III with LPHB beats, there is a tiny-but-present initial q wave — but with pure RBBB beats in lead III there is no such initial q wave. This is precisely what is supposed to happen when you have isolated LPHB. Similarly, in lead V1, there is a tiny-but-present initial r wave for pure RBBB beats — but this initial tiny r wave is lost with LPHB beats in V1. And then in V2,V3 the R wave is decidedly taller with the LPHB beats — which is as expected (the only functioning fascicle is the LAH, so the QRS is more positive in V2,V3 reflection more anterior depolarization that is no longer opposed by the block LPH).
Ken
|
Hi,
ReplyDeleteIn the last ECG you said that ST depression is consistent with ischemia. Isn't it atrial repol instead?
thanks
Olivier, you are correct in leads II, III, aVF. But V3 and V4 and definitely ischemic ST depression. The ST segment is too depressed for atrial repol and, more importantly, far more depressed than the PR segment.
DeleteBut good observation about inferior leads!
Steve